Challenges and way forward for implementation of sugar taxation in the Middle East and North Africa (MENA)
Abstract
Background
Over consumption of added sugar beyond the World Health Organization (WHO) recommended level of 10% of daily energy intake has well-established negative health consequences including oral diseases. However, the average consumption of added sugar in the Middle East and North Africa region (MENA—World Bank's regional classification) is 70% higher than the WHO recommended level. Imposing taxes on added sugar has been proposed by the WHO to decrease its consumption. Yet, only 21.6% of the total MENA population are covered by taxation policies targeting added sugar.
Challenges
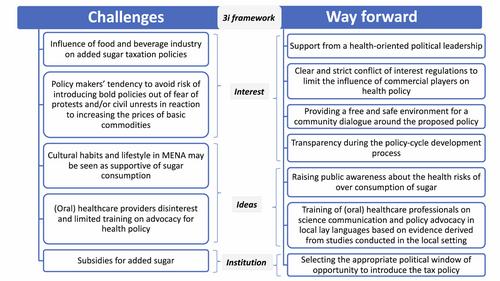
Well-recognized challenges for the implementation of sugar taxation in MENA include the tactics used by the food and beverage industry to block these type of policies. However, there are also other unfamiliar hurdles specific to MENA. Historically, there have been incidents of protest and riots partially sparked by increased price of basic commodities, including sugar, in MENA countries. This may affect the readiness of policy makers in the region to impose added sugar taxes. In addition, there are also cultural, lifestyle and consumption behavioural barriers to implementing added sugar taxation. Ultra-processed foods and sugar-sweetened-beverages (SSBs) rich in added sugar are perceived by many in MENA as essential treats regardless of their health risks. Furthermore, some countries even provide subsidies for added sugar. Also, (oral) healthcare providers generally do not engage in policy advocacy mainly due to limited training on health policy.
Ways forward
Here, we discuss these challenges and suggest some ways forward such as (1) support from a health-oriented political leadership, (2) raising public awareness about the health risks of over consumption of sugar, (3) transparency during the policy-cycle development process, (4) providing a free and safe environment for a community dialogue around the proposed policy, (5) training of (oral) healthcare professionals on science communication and policy advocacy in local lay language/dialect, ideally evidence informed from local/regional studies, (6) selecting the appropriate political window of opportunity to introduce a sugar tax policy, and (7) clear and strict conflict of interest regulations to limit the influence of commercial players on health policy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


