Let's get physical: Aerobic capacity, muscle strength, and muscle endurance after pediatric heart transplantation
IF 1.2
4区 医学
Q3 PEDIATRICS
引用次数: 0
Abstract
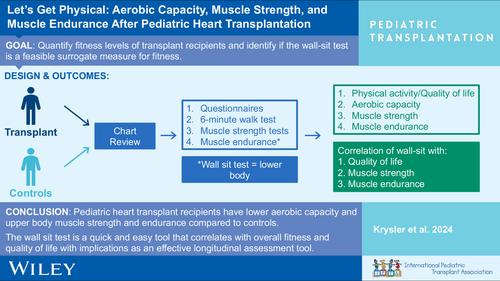
BackgroundPediatric heart (HTx) and kidney transplant (KTx) recipients may have lower physical fitness than healthy children. This study sought to quantify fitness levels in transplant recipients, investigate associations to clinical factors and quality of life, and identify whether a quick, simple wall‐sit test is feasible as a surrogate for overall fitness for longitudinal assessment.MethodsAerobic capacity (6‐min walk test, 6MWT), normalized muscle strength, muscle endurance, physical activity questionnaire (PAQ), and quality of life (PedsQL™) were prospectively assessed in transplanted children and matched healthy controls.ResultsTwenty‐two HTx were compared to 20 controls and 6 KTx. 6MWT %predicted was shorter in HTx (87.2 [69.9–118.6] %) than controls (99.9 [80.4–120] %), but similar to KTx (90.3 [78.6–115] %). Muscle strength was lower in HTx deltoids (6.15 [4.35–11.3] kg/m
让我们运动起来小儿心脏移植后的有氧运动能力、肌肉力量和肌肉耐力
背景小儿心脏(HTx)和肾脏移植(KTx)受者的体能可能低于健康儿童。本研究旨在量化移植受者的体能水平,调查其与临床因素和生活质量的关系,并确定快速、简单的壁坐测试是否可以作为纵向评估整体体能的替代指标。方法对移植儿童和匹配的健康对照组的有氧能力(6 分钟步行测试,6MWT)、归一化肌力、肌耐力、体力活动问卷(PAQ)和生活质量(PedsQL™)进行前瞻性评估。HTx 的 6MWT 预测百分比(87.2 [69.9-118.6] %)短于对照组(99.9 [80.4-120] %),但与 KTx(90.3 [78.6-115] %)相似。与对照组相比,HTx 三角肌(6.15 [4.35-11.3] kg/m2)和 KTx 股四头肌(9.27 [8.65-19.1] kg/m2)的肌肉力量较低。同样,与对照组相比,HTx 俯卧撑(28.6 [0-250] %预测值)、KTx 俯卧撑(8.35 [0-150] %预测值)、HTx 卷发(115 [0-450] %预测值)和 KTx 坐墙时间(18.5 [10.0-54.0] 秒)的肌肉耐力也较低。与只有 9% 的 HTx 相反,所有 KTx 都在接受类固醇治疗。坐墙测试与其他体能参数(归一化股四头肌力量 R = .31、#push-ups R = .39、#curl-ups R = .43)和 PedsQL™ (R = .36)有明显相关性。方便的壁坐测试与体能和报告的生活质量相关,因此可作为纵向评估的有用简便常规方法。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Pediatric Transplantation
医学-小儿科
CiteScore
2.90
自引率
15.40%
发文量
216
审稿时长
3-8 weeks
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


