Range of international surgical strategies for adolescent idiopathic scoliosis: Evaluation of a multi-center survey
Abstract
Background
Surgical treatment of adolescent idiopathic scoliosis (AIS) is very complex and modern instrumentation techniques offer multiple possibilities. Despite numerous publications, there is no clear consensus on the optimal strategy for the correction of scoliotic deformities. The goal of this study was to summarize the current surgical strategies for specific AIS cases within various countries.
Method
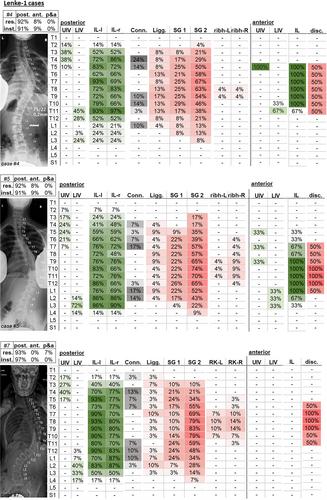
Thirty-two experienced scoliosis surgeons from 15 countries were asked to plan surgeries on 12 representative AIS cases. All AIS cases had an indication for surgery. A questionnaire was provided to document surgical planning. The surgeons were provided with the patients' age and sex, together with radiographs in the lateral and sagittal planes during upright standing and in lateral bending to the left and right, as well as with clinical images. The angles of the main spinal curvatures were specified in the questionnaire. The surgeons were asked to specify their preferred classification system, their surgical approach, the planned fusion length, the type of implants, the rod type, and the resection steps. The data were analyzed with respect to the inter-rater variability, which was quantified using the Fleiss-Kappa Method.
Results
There was a good agreement (k = 0.61) between the surgeons in choosing the Lenke curve type, and a moderate agreement for the lumbar (0.41) and sagittal (0.56) modifiers. The most frequently planned resection procedure was complete facetectomy (67%). The posterior approach was the most commonly (91%) selected strategy to treat AIS. Anterior approaches were chosen most for Lenke 5 type with a rate of 20%. The upper instrumented vertebra (UIV) varied most for Lenke 1, 5, and 6 cases, with a vertebral level discrepancy of up to 10 levels at Lenke 6. The lowest instrumented vertebra varied most for Lenke 1 and 4 by up to five levels. Polyaxial screws were chosen most (56%), followed by monoaxial (20%) and uniplanar (19%) screws and hooks (5%).
Conclusions
The results highlight the commonalities and discrepancy in the surgical treatment of AIS in between surgeons. The selected LIV and UIV can vary depending on the curve type and surgeon. Hook constructs appear to be generally replaced by transpedicular screws. The survey indicates open questions in the AIS treatment and in the understanding of scoliosis biomechanics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


