{"title":"Medial pontine mid-tegmentum syndrome","authors":"Junpei Komagamine, Satsuki Yoshihara, Yasuhiro Kano","doi":"10.1002/ams2.948","DOIUrl":null,"url":null,"abstract":"<p>A 74-year-old man presented to the emergency department with acute diplopia and transient left-sided paresthesia of the upper and lower limbs. He reported no headaches, dizziness, or vision loss. Upon presentation, he was alert and oriented. Neurological examination revealed right abducens nerve palsy with diplopia on the right lateral gaze (Figure 1A). His left-sided paresthesia had improved on presentation, and there were no other neurological findings. Brain magnetic resonance imaging (MRI) revealed a small infarct in the right pontine tegmentum (Figure 1B,C). Magnetic resonance angiography revealed no significant stenosis of the cerebral arteries. Dual antiplatelet therapy was started, and his right abducens nerve palsy gradually resolved. He was discharged after a one-week hospital stay.</p><p>To our knowledge, this is the second report of medial pontine mid-tegmentum syndrome<span><sup>1</sup></span> resulting from damage to the mid-lateral portion of the medial lemniscus of the pons. Because the abducens nerve crosses the medial lemniscus at the pontine level, this syndrome is associated with ipsilateral abducens nerve palsy and contralateral sensory disturbance<span><sup>1</sup></span> (Figure 1D). Given the limited sensitivity of MRI for detecting ischemic stroke of the posterior circulation,<span><sup>2</sup></span> recognition of this syndrome as one of the stroke syndromes is critical for prompt intervention.</p><p>The authors declare no conflicts of interest.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: Informed consent was obtained from the patient.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.948","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.948","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
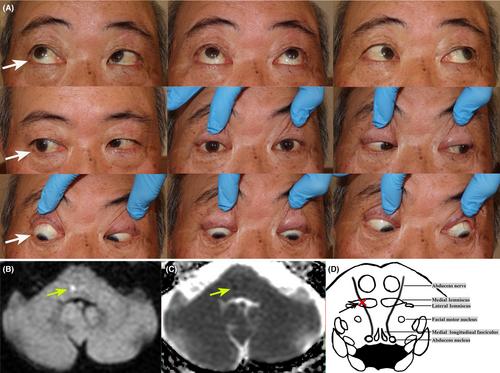
A 74-year-old man presented to the emergency department with acute diplopia and transient left-sided paresthesia of the upper and lower limbs. He reported no headaches, dizziness, or vision loss. Upon presentation, he was alert and oriented. Neurological examination revealed right abducens nerve palsy with diplopia on the right lateral gaze (Figure 1A). His left-sided paresthesia had improved on presentation, and there were no other neurological findings. Brain magnetic resonance imaging (MRI) revealed a small infarct in the right pontine tegmentum (Figure 1B,C). Magnetic resonance angiography revealed no significant stenosis of the cerebral arteries. Dual antiplatelet therapy was started, and his right abducens nerve palsy gradually resolved. He was discharged after a one-week hospital stay.
To our knowledge, this is the second report of medial pontine mid-tegmentum syndrome1 resulting from damage to the mid-lateral portion of the medial lemniscus of the pons. Because the abducens nerve crosses the medial lemniscus at the pontine level, this syndrome is associated with ipsilateral abducens nerve palsy and contralateral sensory disturbance1 (Figure 1D). Given the limited sensitivity of MRI for detecting ischemic stroke of the posterior circulation,2 recognition of this syndrome as one of the stroke syndromes is critical for prompt intervention.
The authors declare no conflicts of interest.
Approval of the research protocol: N/A.
Informed consent: Informed consent was obtained from the patient.
Registry and the registration no. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


