Role of Postoperative Radiotherapy on High-Risk Stage pIIIA-N2 Non-Small Cell Lung Cancer Patients After Complete Resection and Adjuvant Chemotherapy: A Retrospective Cohort Study.
Zu Yi Chen, Huan Wei Liang, Yang Liu, Wei Huang, Xin Bin Pan
{"title":"Role of Postoperative Radiotherapy on High-Risk Stage pIIIA-N2 Non-Small Cell Lung Cancer Patients After Complete Resection and Adjuvant Chemotherapy: A Retrospective Cohort Study.","authors":"Zu Yi Chen, Huan Wei Liang, Yang Liu, Wei Huang, Xin Bin Pan","doi":"10.14740/wjon1832","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of the study was to assess the effectiveness of postoperative radiotherapy in high-risk patients with stage pIIIA-N2 non-small cell lung cancer (NSCLC) following complete resection and adjuvant chemotherapy.</p><p><strong>Methods: </strong>Data from NSCLC patients within the Surveillance, Epidemiology, and End Results (SEER) database were analyzed. The study examined the association between lymph node ratio (LNR) and both cancer-specific survival (CSS) and overall survival (OS) using restricted cubic spline curves. Patients were categorized into high- and low-risk groups based on established LNR cut-off values, and survival outcomes were compared between those receiving postoperative radiotherapy and those who did not within the high-risk group.</p><p><strong>Results: </strong>The study included 1,690 patients. An LNR threshold of 0.29 was identified for both CSS and OS. Patients with an LNR ≥ 0.29 demonstrated significantly worse CSS (hazard ratio (HR) = 1.56, 95% confidence interval (CI): 1.37 - 1.78; P < 0.001) and OS (HR = 1.44, 95% CI: 1.28 - 1.62; P < 0.001) compared to those with an LNR < 0.29. In the high-risk group (LNR ≥ 0.29), postoperative radiotherapy did not significantly affect CSS (HR = 0.98, 95% CI: 0.82 - 1.17; P = 0.809) or OS (HR = 0.95, 95% CI: 0.81 - 1.11; P = 0.533).</p><p><strong>Conclusions: </strong>LNR is a significant prognostic factor in patients with stage pIIIA-N2 NSCLC post complete resection and adjuvant chemotherapy. A higher LNR (≥ 0.29) is associated with poorer CSS and OS. However, postoperative radiotherapy does not confer survival benefits in these high-risk patients. Our findings suggest that postoperative radiotherapy should not be routinely performed in this subgroup. Further research is required to explore effective treatment strategies for these patients.</p>","PeriodicalId":46797,"journal":{"name":"World Journal of Oncology","volume":"15 2","pages":"309-318"},"PeriodicalIF":2.2000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10965260/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/wjon1832","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aim of the study was to assess the effectiveness of postoperative radiotherapy in high-risk patients with stage pIIIA-N2 non-small cell lung cancer (NSCLC) following complete resection and adjuvant chemotherapy.
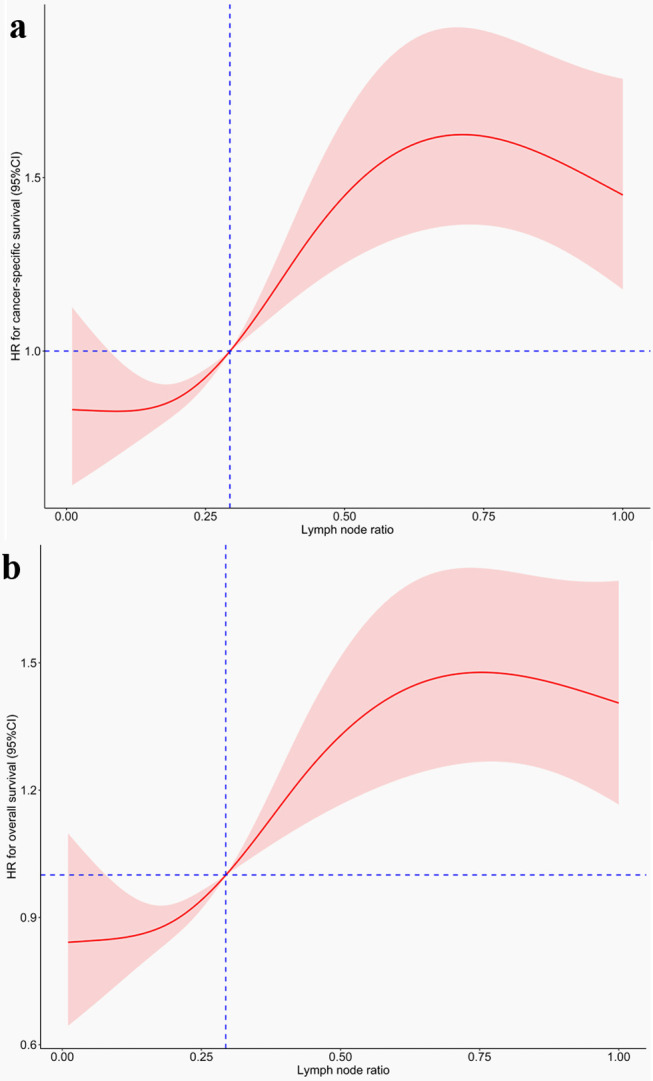
Methods: Data from NSCLC patients within the Surveillance, Epidemiology, and End Results (SEER) database were analyzed. The study examined the association between lymph node ratio (LNR) and both cancer-specific survival (CSS) and overall survival (OS) using restricted cubic spline curves. Patients were categorized into high- and low-risk groups based on established LNR cut-off values, and survival outcomes were compared between those receiving postoperative radiotherapy and those who did not within the high-risk group.
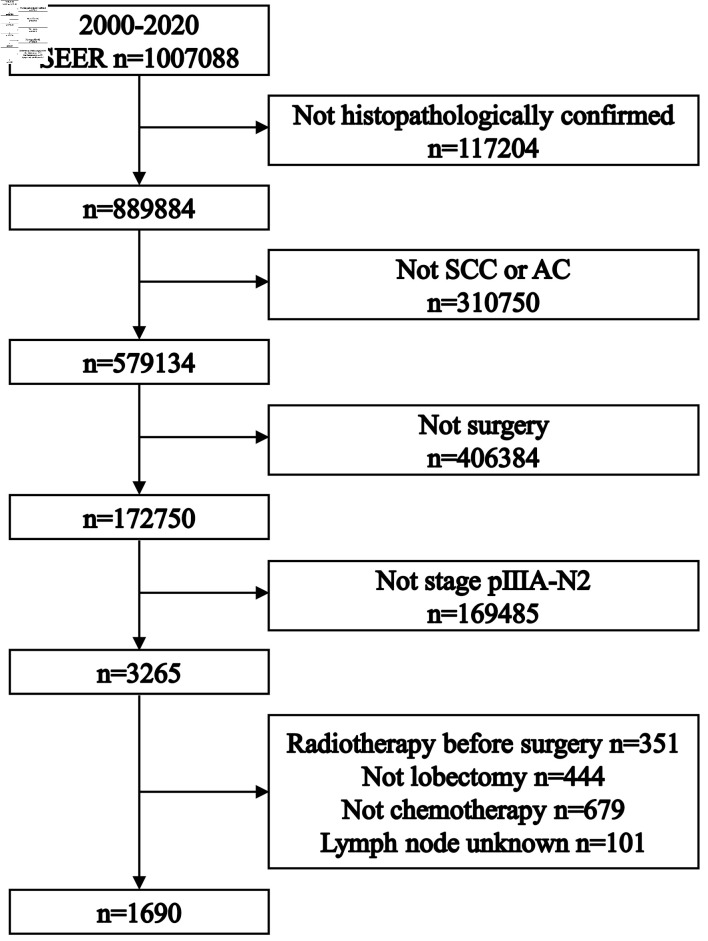
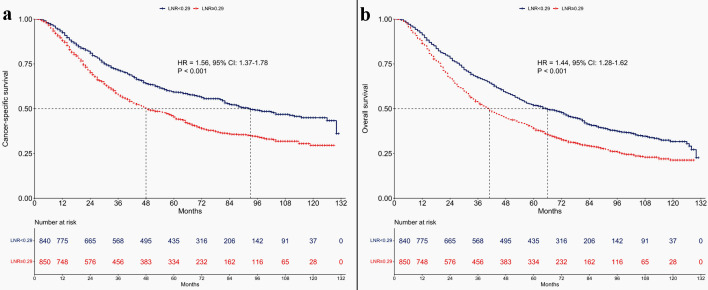
Results: The study included 1,690 patients. An LNR threshold of 0.29 was identified for both CSS and OS. Patients with an LNR ≥ 0.29 demonstrated significantly worse CSS (hazard ratio (HR) = 1.56, 95% confidence interval (CI): 1.37 - 1.78; P < 0.001) and OS (HR = 1.44, 95% CI: 1.28 - 1.62; P < 0.001) compared to those with an LNR < 0.29. In the high-risk group (LNR ≥ 0.29), postoperative radiotherapy did not significantly affect CSS (HR = 0.98, 95% CI: 0.82 - 1.17; P = 0.809) or OS (HR = 0.95, 95% CI: 0.81 - 1.11; P = 0.533).
Conclusions: LNR is a significant prognostic factor in patients with stage pIIIA-N2 NSCLC post complete resection and adjuvant chemotherapy. A higher LNR (≥ 0.29) is associated with poorer CSS and OS. However, postoperative radiotherapy does not confer survival benefits in these high-risk patients. Our findings suggest that postoperative radiotherapy should not be routinely performed in this subgroup. Further research is required to explore effective treatment strategies for these patients.
期刊介绍:
World Journal of Oncology, bimonthly, publishes original contributions describing basic research and clinical investigation of cancer, on the cellular, molecular, prevention, diagnosis, therapy and prognosis aspects. The submissions can be basic research or clinical investigation oriented. This journal welcomes those submissions focused on the clinical trials of new treatment modalities for cancer, and those submissions focused on molecular or cellular research of the oncology pathogenesis. Case reports submitted for consideration of publication should explore either a novel genomic event/description or a new safety signal from an oncolytic agent. The areas of interested manuscripts are these disciplines: tumor immunology and immunotherapy; cancer molecular pharmacology and chemotherapy; drug sensitivity and resistance; cancer epidemiology; clinical trials; cancer pathology; radiobiology and radiation oncology; solid tumor oncology; hematological malignancies; surgical oncology; pediatric oncology; molecular oncology and cancer genes; gene therapy; cancer endocrinology; cancer metastasis; prevention and diagnosis of cancer; other cancer related subjects. The types of manuscripts accepted are original article, review, editorial, short communication, case report, letter to the editor, book review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


