Frederik Pagh Bredahl Kristensen, Erzsébet Horváth-Puhó, Szimonetta Komjáthiné Szépligeti, Frederikke Schoenfeldt Troelsen, Henrik Toft Sørensen
{"title":"Risk of Bleeding and Venous Thromboembolism after Colorectal Cancer Surgery in Patients with and without Type 2 Diabetes: A Danish Cohort Study.","authors":"Frederik Pagh Bredahl Kristensen, Erzsébet Horváth-Puhó, Szimonetta Komjáthiné Szépligeti, Frederikke Schoenfeldt Troelsen, Henrik Toft Sørensen","doi":"10.1055/a-2275-9590","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Bleeding and venous thromboembolism (VTE) are adverse outcomes after colorectal cancer (CRC) surgery. Type 2 diabetes (T2D) clusters with bleeding and VTE risk factors. We examined the bleeding and VTE risk in patients with T2D undergoing CRC surgery and the prognosis after these adverse outcomes. <b>Methods</b> We conducted a prognostic population-based cohort study of 48,295 patients with and without T2D undergoing surgery for incident CRC during 2005 to 2019. Patients with T2D were diagnosed in a hospital setting or had redeemed a glucose-lowering drug prescription; the remaining cohort was patients without diabetes. We estimated the 30-day and 1-year risks of bleeding and VTE and used a Fine-Gray model to compute age-, sex-, and calendar year-adjusted subdistribution hazard ratios (SHRs). The Kaplan-Meier method was used to calculate 1-year mortality after bleeding or VTE. <b>Results</b> Within 30 days after CRC surgery, the risk of bleeding was 2.7% in patients with T2D and 2.0% in patients without diabetes (SHR: 1.30 [95% confidence interval [CI]: 1.10-1.53]). For VTE, the 30-day risks were 0.6% for patients with T2D and 0.6% for patients without diabetes (SHR: 1.01 [95% CI: 0.71-1.42]). The SHRs for bleeding and VTE within 1 year after CRC surgery were similar. The 1-year mortality was 26.0% versus 24.9% in the bleeding cohort and 25.8% versus 27.5% in the VTE cohort for patients with T2D versus without diabetes, respectively. <b>Conclusion</b> Although absolute risks were low, patients with T2D have an increased risk of bleeding but not VTE after CRC surgery.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"8 1","pages":"e146-e154"},"PeriodicalIF":1.8000,"publicationDate":"2024-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10965306/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2275-9590","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
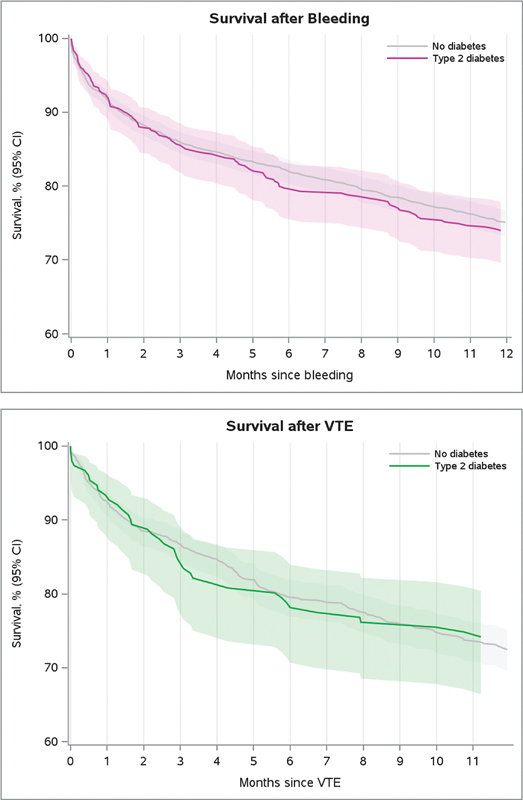
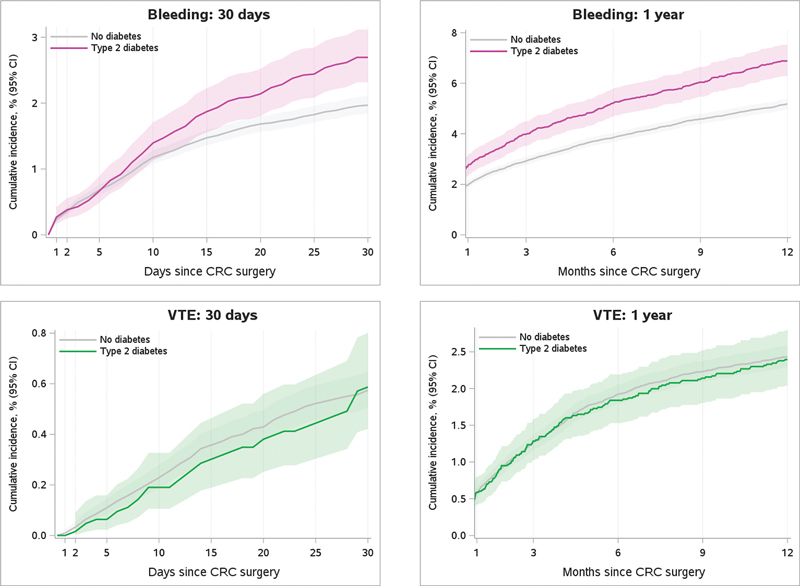
Background Bleeding and venous thromboembolism (VTE) are adverse outcomes after colorectal cancer (CRC) surgery. Type 2 diabetes (T2D) clusters with bleeding and VTE risk factors. We examined the bleeding and VTE risk in patients with T2D undergoing CRC surgery and the prognosis after these adverse outcomes. Methods We conducted a prognostic population-based cohort study of 48,295 patients with and without T2D undergoing surgery for incident CRC during 2005 to 2019. Patients with T2D were diagnosed in a hospital setting or had redeemed a glucose-lowering drug prescription; the remaining cohort was patients without diabetes. We estimated the 30-day and 1-year risks of bleeding and VTE and used a Fine-Gray model to compute age-, sex-, and calendar year-adjusted subdistribution hazard ratios (SHRs). The Kaplan-Meier method was used to calculate 1-year mortality after bleeding or VTE. Results Within 30 days after CRC surgery, the risk of bleeding was 2.7% in patients with T2D and 2.0% in patients without diabetes (SHR: 1.30 [95% confidence interval [CI]: 1.10-1.53]). For VTE, the 30-day risks were 0.6% for patients with T2D and 0.6% for patients without diabetes (SHR: 1.01 [95% CI: 0.71-1.42]). The SHRs for bleeding and VTE within 1 year after CRC surgery were similar. The 1-year mortality was 26.0% versus 24.9% in the bleeding cohort and 25.8% versus 27.5% in the VTE cohort for patients with T2D versus without diabetes, respectively. Conclusion Although absolute risks were low, patients with T2D have an increased risk of bleeding but not VTE after CRC surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


