{"title":"Multicenter randomized controlled trial of intensive uric acid lowering therapy for CKD patients with hyperuricemia: TARGET-UA.","authors":"Tetsuya Yamamoto, Masato Kasahara, Kenji Ueshima, Shiro Uemura, Naoki Kashihara, Kenjiro Kimura, Tsuneo Konta, Tetsuo Shoji, Akira Mima, Masashi Mukoyama, Yoshihiko Saito","doi":"10.1007/s10157-024-02483-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We investigate whether Intensive uric acid (UA)-lowering therapy (ULT) provides increased renal protection compared with standard therapy in chronic kidney disease (CKD) patients.</p><p><strong>Methods: </strong>This was a multicenter randomized controlled trial. Only CKD patients with hyperuricemia were included in this study. The participants were randomly assigned to either the Intensive therapy group (target serum UA level ≥ 4.0 mg/dL and < 5.0 mg/dL) or the standard therapy group (serum UA level ≥ 6.0 mg/dL and < 7.0 mg/dL). ULT was performed using topiroxostat, a non-purine-type selective xanthine oxidase inhibitor. The primary endpoint was change in the logarithmic value of urine albumin to the creatinine ratio (ACR) between baseline and week 52 of the treatment.</p><p><strong>Results: </strong>Three hundred fifty-two patients were included in the full analysis set. In the Standard therapy group, mean serum UA was 8.23 mg/dL at baseline and 6.13 mg/dL at 52 weeks. In the Intensive therapy group, mean serum UA was 8.15 mg/dL at baseline and 5.25 mg/dL at 52 weeks. There was no significant difference in changes in log ACR at 52 weeks between the Intensive therapy and the Standard therapy groups.</p><p><strong>Conclusion: </strong>This study did not reveal the benefit of Intensive ULT to improve albuminuria levels. (UMIN000026741 and jRCTs051180146).</p>","PeriodicalId":10349,"journal":{"name":"Clinical and Experimental Nephrology","volume":" ","pages":"764-772"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11266370/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10157-024-02483-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/26 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We investigate whether Intensive uric acid (UA)-lowering therapy (ULT) provides increased renal protection compared with standard therapy in chronic kidney disease (CKD) patients.
Methods: This was a multicenter randomized controlled trial. Only CKD patients with hyperuricemia were included in this study. The participants were randomly assigned to either the Intensive therapy group (target serum UA level ≥ 4.0 mg/dL and < 5.0 mg/dL) or the standard therapy group (serum UA level ≥ 6.0 mg/dL and < 7.0 mg/dL). ULT was performed using topiroxostat, a non-purine-type selective xanthine oxidase inhibitor. The primary endpoint was change in the logarithmic value of urine albumin to the creatinine ratio (ACR) between baseline and week 52 of the treatment.
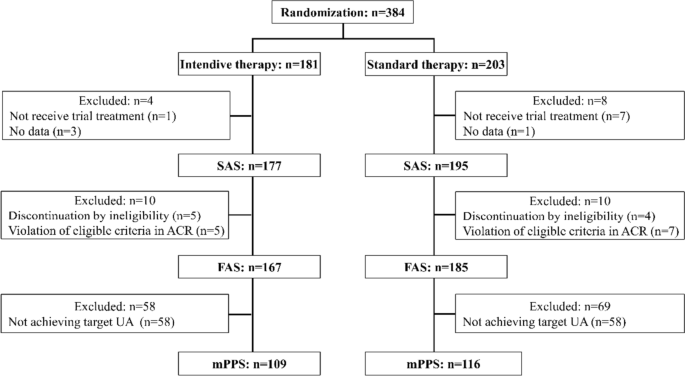
Results: Three hundred fifty-two patients were included in the full analysis set. In the Standard therapy group, mean serum UA was 8.23 mg/dL at baseline and 6.13 mg/dL at 52 weeks. In the Intensive therapy group, mean serum UA was 8.15 mg/dL at baseline and 5.25 mg/dL at 52 weeks. There was no significant difference in changes in log ACR at 52 weeks between the Intensive therapy and the Standard therapy groups.
Conclusion: This study did not reveal the benefit of Intensive ULT to improve albuminuria levels. (UMIN000026741 and jRCTs051180146).
期刊介绍:
Clinical and Experimental Nephrology is a peer-reviewed monthly journal, officially published by the Japanese Society of Nephrology (JSN) to provide an international forum for the discussion of research and issues relating to the study of nephrology. Out of respect for the founders of the JSN, the title of this journal uses the term “nephrology,” a word created and brought into use with the establishment of the JSN (Japanese Journal of Nephrology, Vol. 2, No. 1, 1960). The journal publishes articles on all aspects of nephrology, including basic, experimental, and clinical research, so as to share the latest research findings and ideas not only with members of the JSN, but with all researchers who wish to contribute to a better understanding of recent advances in nephrology. The journal is unique in that it introduces to an international readership original reports from Japan and also the clinical standards discussed and agreed by JSN.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


