Predictors and outcomes of withholding and withdrawal of life-sustaining treatments in intensive care units in Singapore: a multicentre observational study.
Clare Fong, Wern Lunn Kueh, Sennen Jin Wen Lew, Benjamin Choon Heng Ho, Yu-Lin Wong, Yie Hui Lau, Yew Woon Chia, Hui Ling Tan, Ying Hao Christopher Seet, Wen Ting Siow, Graeme MacLaren, Rohit Agrawal, Tian Jin Lim, Shir Lynn Lim, Toon Wei Lim, Vui Kian Ho, Chai Rick Soh, Duu Wen Sewa, Chian Min Loo, Faheem Ahmed Khan, Chee Keat Tan, Roshni Sadashiv Gokhale, Chuin Siau, Noelle Louise Siew Hua Lim, Chik-Foo Yim, Jonathen Venkatachalam, Kumaresh Venkatesan, Naville Chi Hock Chia, Mei Fong Liew, Guihong Li, Li Li, Su Mon Myat, Zena Zena, Shuling Zhuo, Ling Ling Yueh, Caroline Shu Fang Tan, Jing Ma, Siew Lian Yeo, Yiong Huak Chan, Jason Phua
{"title":"Predictors and outcomes of withholding and withdrawal of life-sustaining treatments in intensive care units in Singapore: a multicentre observational study.","authors":"Clare Fong, Wern Lunn Kueh, Sennen Jin Wen Lew, Benjamin Choon Heng Ho, Yu-Lin Wong, Yie Hui Lau, Yew Woon Chia, Hui Ling Tan, Ying Hao Christopher Seet, Wen Ting Siow, Graeme MacLaren, Rohit Agrawal, Tian Jin Lim, Shir Lynn Lim, Toon Wei Lim, Vui Kian Ho, Chai Rick Soh, Duu Wen Sewa, Chian Min Loo, Faheem Ahmed Khan, Chee Keat Tan, Roshni Sadashiv Gokhale, Chuin Siau, Noelle Louise Siew Hua Lim, Chik-Foo Yim, Jonathen Venkatachalam, Kumaresh Venkatesan, Naville Chi Hock Chia, Mei Fong Liew, Guihong Li, Li Li, Su Mon Myat, Zena Zena, Shuling Zhuo, Ling Ling Yueh, Caroline Shu Fang Tan, Jing Ma, Siew Lian Yeo, Yiong Huak Chan, Jason Phua","doi":"10.1186/s40560-024-00725-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clinical practice guidelines on limitation of life-sustaining treatments (LST) in the intensive care unit (ICU), in the form of withholding or withdrawal of LST, state that there is no ethical difference between the two. Such statements are not uniformly accepted worldwide, and there are few studies on LST limitation in Asia. This study aimed to evaluate the predictors and outcomes of withholding and withdrawal of LST in Singapore, focusing on the similarities and differences between the two approaches.</p><p><strong>Methods: </strong>This was a multicentre observational study of patients admitted to 21 adult ICUs across 9 public hospitals in Singapore over an average of three months per year from 2014 to 2019. The primary outcome measures were withholding and withdrawal of LST (cardiopulmonary resuscitation, invasive mechanical ventilation, and vasopressors/inotropes). The secondary outcome measure was hospital mortality. Multivariable generalised mixed model analysis was used to identify independent predictors for withdrawal and withholding of LST and if LST limitation predicts hospital mortality.</p><p><strong>Results: </strong>There were 8907 patients and 9723 admissions. Of the former, 80.8% had no limitation of LST, 13.0% had LST withheld, and 6.2% had LST withdrawn. Common independent predictors for withholding and withdrawal were increasing age, absence of chronic kidney dialysis, greater dependence in activities of daily living, cardiopulmonary resuscitation before ICU admission, higher Acute Physiology and Chronic Health Evaluation (APACHE) II score, and higher level of care in the first 24 h of ICU admission. Additional predictors for withholding included being of Chinese race, the religions of Hinduism and Islam, malignancy, and chronic liver failure. The additional predictor for withdrawal was lower hospital paying class (with greater government subsidy for hospital bills). Hospital mortality in patients without LST limitation, with LST withholding, and with LST withdrawal was 10.6%, 82.1%, and 91.8%, respectively (p < 0.001). Withholding (odds ratio 13.822, 95% confidence interval 9.987-19.132) and withdrawal (odds ratio 38.319, 95% confidence interval 24.351-60.298) were both found to be independent predictors of hospital mortality on multivariable analysis.</p><p><strong>Conclusions: </strong>Differences in the independent predictors of withholding and withdrawal of LST exist. Even after accounting for baseline characteristics, both withholding and withdrawal of LST independently predict hospital mortality. Later mortality in patients who had LST withdrawn compared to withholding suggests that the decision to withdraw may be at the point when medical futility is recognised.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"12 1","pages":"13"},"PeriodicalIF":4.7000,"publicationDate":"2024-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10964634/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-024-00725-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Clinical practice guidelines on limitation of life-sustaining treatments (LST) in the intensive care unit (ICU), in the form of withholding or withdrawal of LST, state that there is no ethical difference between the two. Such statements are not uniformly accepted worldwide, and there are few studies on LST limitation in Asia. This study aimed to evaluate the predictors and outcomes of withholding and withdrawal of LST in Singapore, focusing on the similarities and differences between the two approaches.
Methods: This was a multicentre observational study of patients admitted to 21 adult ICUs across 9 public hospitals in Singapore over an average of three months per year from 2014 to 2019. The primary outcome measures were withholding and withdrawal of LST (cardiopulmonary resuscitation, invasive mechanical ventilation, and vasopressors/inotropes). The secondary outcome measure was hospital mortality. Multivariable generalised mixed model analysis was used to identify independent predictors for withdrawal and withholding of LST and if LST limitation predicts hospital mortality.
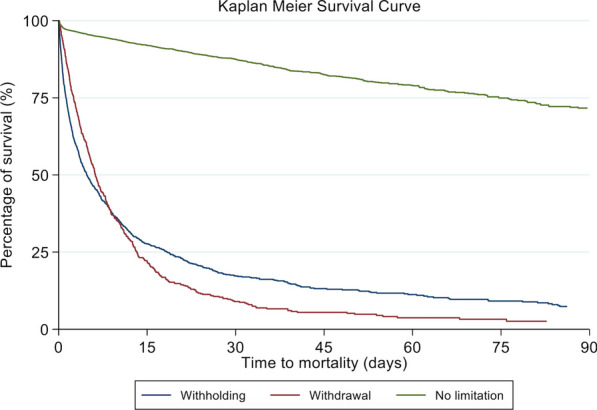
Results: There were 8907 patients and 9723 admissions. Of the former, 80.8% had no limitation of LST, 13.0% had LST withheld, and 6.2% had LST withdrawn. Common independent predictors for withholding and withdrawal were increasing age, absence of chronic kidney dialysis, greater dependence in activities of daily living, cardiopulmonary resuscitation before ICU admission, higher Acute Physiology and Chronic Health Evaluation (APACHE) II score, and higher level of care in the first 24 h of ICU admission. Additional predictors for withholding included being of Chinese race, the religions of Hinduism and Islam, malignancy, and chronic liver failure. The additional predictor for withdrawal was lower hospital paying class (with greater government subsidy for hospital bills). Hospital mortality in patients without LST limitation, with LST withholding, and with LST withdrawal was 10.6%, 82.1%, and 91.8%, respectively (p < 0.001). Withholding (odds ratio 13.822, 95% confidence interval 9.987-19.132) and withdrawal (odds ratio 38.319, 95% confidence interval 24.351-60.298) were both found to be independent predictors of hospital mortality on multivariable analysis.
Conclusions: Differences in the independent predictors of withholding and withdrawal of LST exist. Even after accounting for baseline characteristics, both withholding and withdrawal of LST independently predict hospital mortality. Later mortality in patients who had LST withdrawn compared to withholding suggests that the decision to withdraw may be at the point when medical futility is recognised.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


