Pei-Pei Jin, Ning Ding, Jing Dai, Xiao-Yan Liu, Pei-Min Mao
{"title":"Effect of Reduced INR in Early Pregnancy on the Occurrence of Preeclampsia: A Retrospective Cohort Study.","authors":"Pei-Pei Jin, Ning Ding, Jing Dai, Xiao-Yan Liu, Pei-Min Mao","doi":"10.1177/10760296241238015","DOIUrl":null,"url":null,"abstract":"<p><p>To investigate the effect of reduced early-pregnancy activated partial thrombin time (APTT), prothrombin time (PT), and international standardized ratio (INR) on the risk of preeclampsia. A total of 8549 pregnant women with singleton births were included. Early pregnancy APTT, PT, and INR levels, with age, birth, prepregnancy body mass index, fibrinogen (FBG), thrombin time (TT), D-dimer (DD2), antithrombin III (ATIII), fibrin degradation products (FDP) as confounders, generalized linear model of APTT, the relative risk of PT and INR when INR reduction. After adequate adjustment for confounders, the relative risk of preeclampsia was 0.703 for every 1 s increase in plasma PT results in early pregnancy, and for every 0.1 increase in plasma INR results, the relative risk of preeclampsia was 0.767. With a PT less than the P25 quantile (<11 s), the relative risk of preeclampsia was 1.328. The relative risk of preeclampsia at an INR less than the P25 quantile (<0.92) was 1.24. There was no statistical association between APTT on the risk of preeclampsia. The relative risk of preeclampsia is strongly associated with a decrease in PT and INR in early pregnancy. PT and INR in early pregnancy were a potential marker in the risk stratification of preeclampsia. Focusing on reduced PT and INR levels in early pregnancy can help to identify early pregnancies at risk for preeclampsia.</p>","PeriodicalId":10335,"journal":{"name":"Clinical and Applied Thrombosis/Hemostasis","volume":"30 ","pages":"10760296241238015"},"PeriodicalIF":2.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10964434/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Applied Thrombosis/Hemostasis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10760296241238015","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
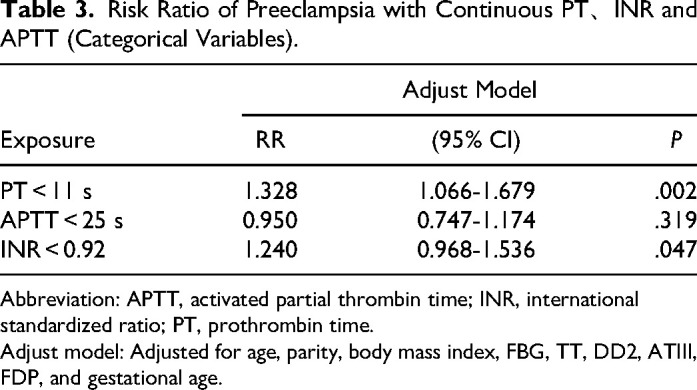
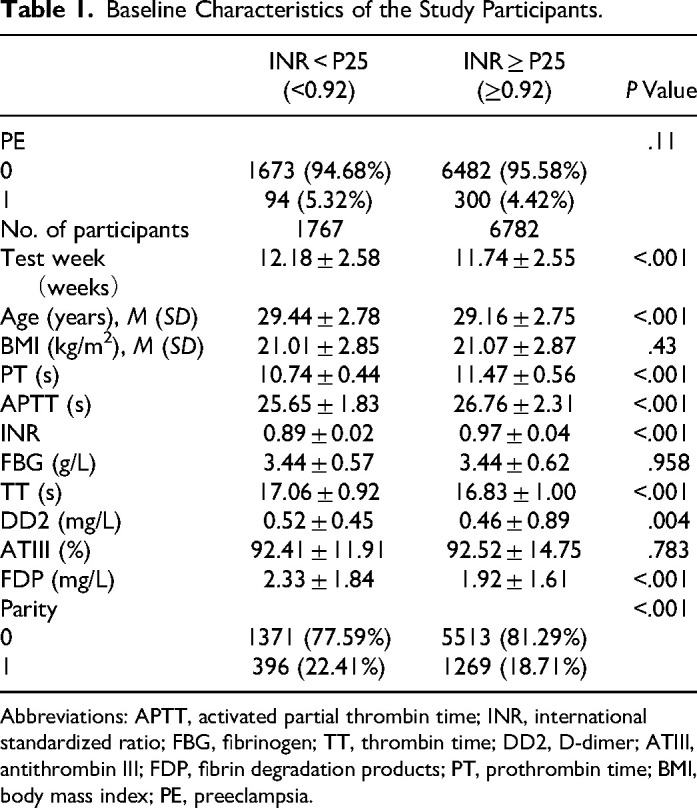
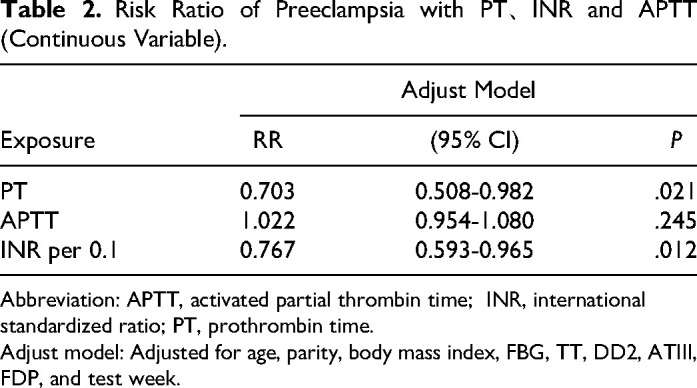
To investigate the effect of reduced early-pregnancy activated partial thrombin time (APTT), prothrombin time (PT), and international standardized ratio (INR) on the risk of preeclampsia. A total of 8549 pregnant women with singleton births were included. Early pregnancy APTT, PT, and INR levels, with age, birth, prepregnancy body mass index, fibrinogen (FBG), thrombin time (TT), D-dimer (DD2), antithrombin III (ATIII), fibrin degradation products (FDP) as confounders, generalized linear model of APTT, the relative risk of PT and INR when INR reduction. After adequate adjustment for confounders, the relative risk of preeclampsia was 0.703 for every 1 s increase in plasma PT results in early pregnancy, and for every 0.1 increase in plasma INR results, the relative risk of preeclampsia was 0.767. With a PT less than the P25 quantile (<11 s), the relative risk of preeclampsia was 1.328. The relative risk of preeclampsia at an INR less than the P25 quantile (<0.92) was 1.24. There was no statistical association between APTT on the risk of preeclampsia. The relative risk of preeclampsia is strongly associated with a decrease in PT and INR in early pregnancy. PT and INR in early pregnancy were a potential marker in the risk stratification of preeclampsia. Focusing on reduced PT and INR levels in early pregnancy can help to identify early pregnancies at risk for preeclampsia.
期刊介绍:
CATH is a peer-reviewed bi-monthly journal that addresses the practical clinical and laboratory issues involved in managing bleeding and clotting disorders, especially those related to thrombosis, hemostasis, and vascular disorders. CATH covers clinical trials, studies on etiology, pathophysiology, diagnosis and treatment of thrombohemorrhagic disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


