{"title":"Omitting Lymph Node Dissection for Small Ground-Glass Opacity-Dominant Tumors.","authors":"Takahiro Mimae, Yoshihiro Miyata, Norifumi Tsubokawa, Yujin Kudo, Takuya Nagashima, Hiroyuki Ito, Norihiko Ikeda, Morihito Okada","doi":"10.1016/j.athoracsur.2024.03.013","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of this study was to determine the optimal extent of lymph node dissection required in patients with small (≤3 cm) radiologically ground-glass opacity-dominant, peripheral, non-small cell lung cancer tumors.</p><p><strong>Methods: </strong>The study analyzed the clinicopathologic findings and surgical outcomes of 988 patients with radiologic, ground-glass opacity-dominant non-small cell lung cancer without lymph node involvement who underwent complete resection of the primary tumor between 2010 and 2020. Patients were followed up for 54.5 months (median). Kaplan-Meier curves and the log-rank test were used in statistical analyses of the prognosis.</p><p><strong>Results: </strong>Median age, whole tumor size, solid tumor size, and maximum standardized uptake values were 68 years, 1.7 cm, 0.4 cm, and 0.9, respectively. Sixty percent of the cohort was female (n = 590). Wedge resection, segmentectomy, and lobectomy were performed in 206, 372, and 410 patients, respectively. A total of 982 of 988 (99%) tumors were adenocarcinomas. One patient had hilar lymph node involvement; however, no mediastinal lymph node metastasis or hilar or mediastinal lymph node recurrence was detected. The 5-year overall survival rate was 96.5% (95% CI, 94.8%-97.7%). Excellent survival outcomes were achieved regardless of procedure (wedge resection, 94.7% [95% CI, 89.1%-97.5%]; segmentectomy, 96.9% [95% CI, 93.7%-98.5%]; and lobectomy, 97.1% [95% CI, 94.4%-98.5%]).</p><p><strong>Conclusions: </strong>Omitting lymph node dissection may be acceptable with curative intent for small tumors with radiologic ground-glass opacity dominance. Appropriate surgical procedures such as wedge resection, segmentectomy, or lobectomy can provide satisfactory outcomes in patients with indolent tumors if surgical margins are secured.</p>","PeriodicalId":50976,"journal":{"name":"Annals of Thoracic Surgery","volume":" ","pages":"192-198"},"PeriodicalIF":3.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.athoracsur.2024.03.013","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The purpose of this study was to determine the optimal extent of lymph node dissection required in patients with small (≤3 cm) radiologically ground-glass opacity-dominant, peripheral, non-small cell lung cancer tumors.
Methods: The study analyzed the clinicopathologic findings and surgical outcomes of 988 patients with radiologic, ground-glass opacity-dominant non-small cell lung cancer without lymph node involvement who underwent complete resection of the primary tumor between 2010 and 2020. Patients were followed up for 54.5 months (median). Kaplan-Meier curves and the log-rank test were used in statistical analyses of the prognosis.
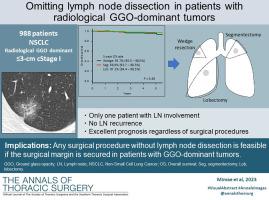
Results: Median age, whole tumor size, solid tumor size, and maximum standardized uptake values were 68 years, 1.7 cm, 0.4 cm, and 0.9, respectively. Sixty percent of the cohort was female (n = 590). Wedge resection, segmentectomy, and lobectomy were performed in 206, 372, and 410 patients, respectively. A total of 982 of 988 (99%) tumors were adenocarcinomas. One patient had hilar lymph node involvement; however, no mediastinal lymph node metastasis or hilar or mediastinal lymph node recurrence was detected. The 5-year overall survival rate was 96.5% (95% CI, 94.8%-97.7%). Excellent survival outcomes were achieved regardless of procedure (wedge resection, 94.7% [95% CI, 89.1%-97.5%]; segmentectomy, 96.9% [95% CI, 93.7%-98.5%]; and lobectomy, 97.1% [95% CI, 94.4%-98.5%]).
Conclusions: Omitting lymph node dissection may be acceptable with curative intent for small tumors with radiologic ground-glass opacity dominance. Appropriate surgical procedures such as wedge resection, segmentectomy, or lobectomy can provide satisfactory outcomes in patients with indolent tumors if surgical margins are secured.
期刊介绍:
The mission of The Annals of Thoracic Surgery is to promote scholarship in cardiothoracic surgery patient care, clinical practice, research, education, and policy. As the official journal of two of the largest American associations in its specialty, this leading monthly enjoys outstanding editorial leadership and maintains rigorous selection standards.
The Annals of Thoracic Surgery features:
• Full-length original articles on clinical advances, current surgical methods, and controversial topics and techniques
• New Technology articles
• Case reports
• "How-to-do-it" features
• Reviews of current literature
• Supplements on symposia
• Commentary pieces and correspondence
• CME
• Online-only case reports, "how-to-do-its", and images in cardiothoracic surgery.
An authoritative, clinically oriented, comprehensive resource, The Annals of Thoracic Surgery is committed to providing a place for all thoracic surgeons to relate experiences which will help improve patient care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


