Federico Franchi, Emanuele Detti, Alberto Fogagnolo, Savino Spadaro, Gabriele Cevenini, Gennaro Cataldo, Tommaso Addabbo, Cesare Biuzzi, Daniele Marianello, Carlo Alberto Volta, Fabio Silvio Taccone, Sabino Scolletta
{"title":"Estimation of the transpulmonary pressure from the central venous pressure in mechanically ventilated patients.","authors":"Federico Franchi, Emanuele Detti, Alberto Fogagnolo, Savino Spadaro, Gabriele Cevenini, Gennaro Cataldo, Tommaso Addabbo, Cesare Biuzzi, Daniele Marianello, Carlo Alberto Volta, Fabio Silvio Taccone, Sabino Scolletta","doi":"10.1007/s10877-024-01150-5","DOIUrl":null,"url":null,"abstract":"<p><p>Transpulmonary pressure (P<sub>L</sub>) calculation requires esophageal pressure (P<sub>ES</sub>) as a surrogate of pleural pressure (Ppl), but its calibration is a cumbersome technique. Central venous pressure (CVP) swings may reflect tidal variations in Ppl and could be used instead of P<sub>ES</sub>, but the interpretation of CVP waveforms could be difficult due to superposition of heartbeat-induced pressure changes. Thus, we developed a digital filter able to remove the cardiac noise to obtain a filtered CVP (f-CVP). The aim of the study was to evaluate the accuracy of CVP and filtered CVP swings (ΔCVP and Δf-CVP, respectively) in estimating esophageal respiratory swings (ΔP<sub>ES</sub>) and compare P<sub>L</sub> calculated with CVP, f-CVP and P<sub>ES;</sub> then we tested the diagnostic accuracy of the f-CVP method to identify unsafe high P<sub>L</sub> levels, defined as P<sub>L</sub>>10 cmH<sub>2</sub>O. Twenty patients with acute respiratory failure (defined as PaO<sub>2</sub>/FiO<sub>2</sub> ratio below 200 mmHg) treated with invasive mechanical ventilation and monitored with an esophageal balloon and central venous catheter were enrolled prospectively. For each patient a recording session at baseline was performed, repeated if a modification in ventilatory settings occurred. P<sub>ES</sub>, CVP and airway pressure during an end-inspiratory and -expiratory pause were simultaneously recorded; CVP, f-CVP and P<sub>ES</sub> waveforms were analyzed off-line and used to calculate transpulmonary pressure (P<sub>L</sub>CVP, P<sub>L</sub>f-CVP, P<sub>L</sub>P<sub>ES</sub>, respectively). Δf-CVP correlated better than ΔCVP with ΔP<sub>ES</sub> (r = 0.8, p = 0.001 vs. r = 0.08, p = 0.73), with a lower bias in Bland Altman analysis in favor of P<sub>L</sub>f-CVP (mean bias - 0.16, Limits of Agreement (LoA) -1.31, 0.98 cmH<sub>2</sub>O vs. mean bias - 0.79, LoA - 3.14, 1.55 cmH<sub>2</sub>O). Both P<sub>L</sub>f-CVP and P<sub>L</sub>CVP correlated well with P<sub>L</sub>P<sub>ES</sub> (r = 0.98, p < 0.001 vs. r = 0.94, p < 0.001), again with a lower bias in Bland Altman analysis in favor of P<sub>L</sub>f-CVP (0.15, LoA - 0.95, 1.26 cmH<sub>2</sub>O vs. 0.80, LoA - 1.51, 3.12, cmH<sub>2</sub>O). P<sub>L</sub>f-CVP discriminated high P<sub>L</sub> value with an area under the receiver operating characteristic curve 0.99 (standard deviation, SD, 0.02) (AUC difference = 0.01 [-0.024; 0.05], p = 0.48). In mechanically ventilated patients with acute respiratory failure, the digital filtered CVP estimated ΔP<sub>ES</sub> and P<sub>L</sub> obtained from digital filtered CVP represented a reliable value of standard P<sub>L</sub> measured with the esophageal method and could identify patients with non-protective ventilation settings.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"847-858"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11297816/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01150-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
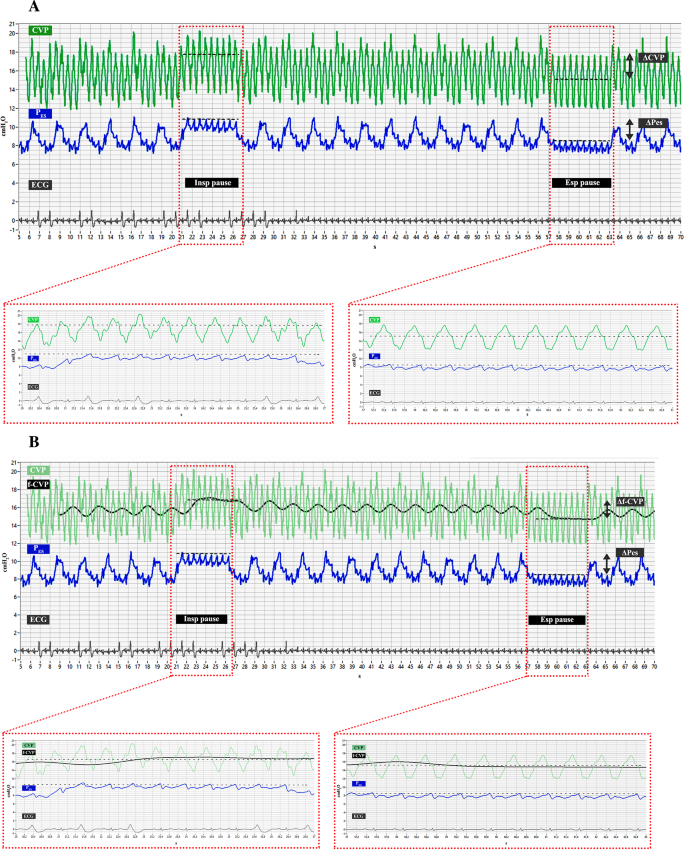
Transpulmonary pressure (PL) calculation requires esophageal pressure (PES) as a surrogate of pleural pressure (Ppl), but its calibration is a cumbersome technique. Central venous pressure (CVP) swings may reflect tidal variations in Ppl and could be used instead of PES, but the interpretation of CVP waveforms could be difficult due to superposition of heartbeat-induced pressure changes. Thus, we developed a digital filter able to remove the cardiac noise to obtain a filtered CVP (f-CVP). The aim of the study was to evaluate the accuracy of CVP and filtered CVP swings (ΔCVP and Δf-CVP, respectively) in estimating esophageal respiratory swings (ΔPES) and compare PL calculated with CVP, f-CVP and PES; then we tested the diagnostic accuracy of the f-CVP method to identify unsafe high PL levels, defined as PL>10 cmH2O. Twenty patients with acute respiratory failure (defined as PaO2/FiO2 ratio below 200 mmHg) treated with invasive mechanical ventilation and monitored with an esophageal balloon and central venous catheter were enrolled prospectively. For each patient a recording session at baseline was performed, repeated if a modification in ventilatory settings occurred. PES, CVP and airway pressure during an end-inspiratory and -expiratory pause were simultaneously recorded; CVP, f-CVP and PES waveforms were analyzed off-line and used to calculate transpulmonary pressure (PLCVP, PLf-CVP, PLPES, respectively). Δf-CVP correlated better than ΔCVP with ΔPES (r = 0.8, p = 0.001 vs. r = 0.08, p = 0.73), with a lower bias in Bland Altman analysis in favor of PLf-CVP (mean bias - 0.16, Limits of Agreement (LoA) -1.31, 0.98 cmH2O vs. mean bias - 0.79, LoA - 3.14, 1.55 cmH2O). Both PLf-CVP and PLCVP correlated well with PLPES (r = 0.98, p < 0.001 vs. r = 0.94, p < 0.001), again with a lower bias in Bland Altman analysis in favor of PLf-CVP (0.15, LoA - 0.95, 1.26 cmH2O vs. 0.80, LoA - 1.51, 3.12, cmH2O). PLf-CVP discriminated high PL value with an area under the receiver operating characteristic curve 0.99 (standard deviation, SD, 0.02) (AUC difference = 0.01 [-0.024; 0.05], p = 0.48). In mechanically ventilated patients with acute respiratory failure, the digital filtered CVP estimated ΔPES and PL obtained from digital filtered CVP represented a reliable value of standard PL measured with the esophageal method and could identify patients with non-protective ventilation settings.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


