Terézia B Andrási, Alannah C Glück, Ildar Talipov, Lachezar Volevski, Ion Vasiloi
{"title":"Sequential composite BIMA grafting for 3v-CAD: factors that predict successful outcome of the one-inflow and two-inflow revascularization techniques.","authors":"Terézia B Andrási, Alannah C Glück, Ildar Talipov, Lachezar Volevski, Ion Vasiloi","doi":"10.1007/s11748-024-02022-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The effect of one-inflow and two-inflow coronary surgical revascularization techniques inclosing skeletonized double mammary artery (BIMA) as T-graft on outcome is studied.</p><p><strong>Methods: </strong>Early ad mid-term outcome of complete BIMA revascularization (C-T-BIMA) versus left-sided BIMA with right-sided aorto-coronary bypass (L-T-BIMA + R-CABG) is quantified and analyzed by multivariate logistic regression, Cox-regression, and Kaplan-Meier analysis in a series of 204 consecutive patients treated for triple-vessel coronary disease (3v-CAD).</p><p><strong>Results: </strong>The L-T-BIMA + R-CABG technique (n = 104) enables higher number of total (4.02 ± 0.87 vs. 3.71 ± 0.69, p = 0.015) and right-sided (1.21 ± 0.43 vs. 1.02 ± 0.32, p = 0.001) coronary anastomoses, improves total bypass flow (125.88 ± 92.41 vs. 82.50 ± 49.26 ml, p < 0.0001) and bypass flow/anastomosis (31.83 ± 23.9 vs.22.77 ± 14.23, p = 0.001), and enhances completeness of revascularization (84% vs.69%, p = 0.014) compared to C-T-BIMA strategy (n = 100), respectively. Although the incidence of MACCE was comparable in the two groups (8% vs.1.2%, p = 0.055), the progression of functional mitral regurgitation (FMR) was significantly lower after L-T-BIMA + R-CABG, then after C-T-BIMA (47% vs.64%, p = 0.017). The use of C-T-BIMA-technique (HR = 4.2, p = 0.01) and preoperative RCA occlusion (HR = 3.006, p = 0.023) predicted FMR progression, whereas L-T-Graft + R-CABG technique protected against it (X<sup>2</sup> = 14.04, p < 0.0001) independent of the anatomic and clinical complexity (Syntax score I: HR = 16.2, p = 0.156, Syntax score II: HR = 1.901, p = 0.751), of early- (0.96% vs.2%, p = 0.617) and mid-term mortality (5.8% vs.4%, p = 0.748) when compared to C-T-BIMA, respectively.</p><p><strong>Conclusions: </strong>The two-inflow coronary revascularization by L-T-BIMA + R-CABG better protects against FMR progression without increasing MACCE and mortality. Older patients with RCA occlusion and reduced LV-EF benefit most from the two-inflow L-T-BIMA + R-CABG technique. Younger 3v-CAD patients with normal LV-EF can preferentially be managed with the one-inflow C-T-BIMA; however, long-term outcome remains to be revealed.</p>","PeriodicalId":12585,"journal":{"name":"General Thoracic and Cardiovascular Surgery","volume":" ","pages":"656-667"},"PeriodicalIF":1.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11402859/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"General Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11748-024-02022-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/20 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The effect of one-inflow and two-inflow coronary surgical revascularization techniques inclosing skeletonized double mammary artery (BIMA) as T-graft on outcome is studied.
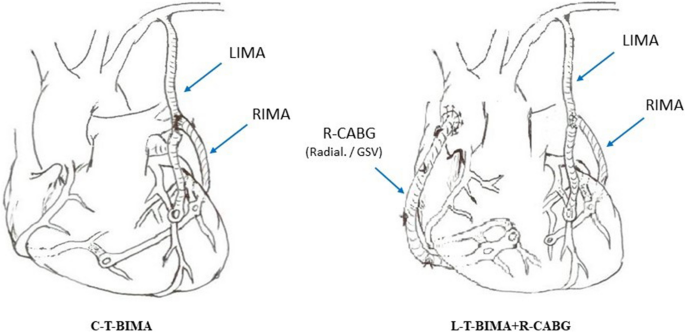
Methods: Early ad mid-term outcome of complete BIMA revascularization (C-T-BIMA) versus left-sided BIMA with right-sided aorto-coronary bypass (L-T-BIMA + R-CABG) is quantified and analyzed by multivariate logistic regression, Cox-regression, and Kaplan-Meier analysis in a series of 204 consecutive patients treated for triple-vessel coronary disease (3v-CAD).
Results: The L-T-BIMA + R-CABG technique (n = 104) enables higher number of total (4.02 ± 0.87 vs. 3.71 ± 0.69, p = 0.015) and right-sided (1.21 ± 0.43 vs. 1.02 ± 0.32, p = 0.001) coronary anastomoses, improves total bypass flow (125.88 ± 92.41 vs. 82.50 ± 49.26 ml, p < 0.0001) and bypass flow/anastomosis (31.83 ± 23.9 vs.22.77 ± 14.23, p = 0.001), and enhances completeness of revascularization (84% vs.69%, p = 0.014) compared to C-T-BIMA strategy (n = 100), respectively. Although the incidence of MACCE was comparable in the two groups (8% vs.1.2%, p = 0.055), the progression of functional mitral regurgitation (FMR) was significantly lower after L-T-BIMA + R-CABG, then after C-T-BIMA (47% vs.64%, p = 0.017). The use of C-T-BIMA-technique (HR = 4.2, p = 0.01) and preoperative RCA occlusion (HR = 3.006, p = 0.023) predicted FMR progression, whereas L-T-Graft + R-CABG technique protected against it (X2 = 14.04, p < 0.0001) independent of the anatomic and clinical complexity (Syntax score I: HR = 16.2, p = 0.156, Syntax score II: HR = 1.901, p = 0.751), of early- (0.96% vs.2%, p = 0.617) and mid-term mortality (5.8% vs.4%, p = 0.748) when compared to C-T-BIMA, respectively.
Conclusions: The two-inflow coronary revascularization by L-T-BIMA + R-CABG better protects against FMR progression without increasing MACCE and mortality. Older patients with RCA occlusion and reduced LV-EF benefit most from the two-inflow L-T-BIMA + R-CABG technique. Younger 3v-CAD patients with normal LV-EF can preferentially be managed with the one-inflow C-T-BIMA; however, long-term outcome remains to be revealed.
期刊介绍:
The General Thoracic and Cardiovascular Surgery is the official publication of The Japanese Association for Thoracic Surgery and The Japanese Association for Chest Surgery, the affiliated journal of The Japanese Society for Cardiovascular Surgery, that publishes clinical and experimental studies in fields related to thoracic and cardiovascular surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


