Kim Vo, Colton Ladbury, Stephanie Yoon, Jose Bazan, Scott Glaser, Arya Amini
{"title":"Omission of adjuvant radiotherapy in low-risk elderly males with breast cancer","authors":"Kim Vo, Colton Ladbury, Stephanie Yoon, Jose Bazan, Scott Glaser, Arya Amini","doi":"10.1007/s12282-024-01560-y","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Purpose</h3><p>Randomized clinical trials demonstrate that lumpectomy + hormone therapy (HT) without radiation therapy (RT) yields equivalent survival and acceptable local–regional outcomes in elderly women with early-stage, node-negative, hormone-receptor positive (HR +) breast cancer. Whether these data apply to men with the same inclusion criteria remains unknown.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>The National Cancer Database was queried for male patients ≥ 65 years with pathologic T1-2N0 (≤ 3 cm) HR + breast cancer treated with breast-conserving surgery with negative margins from 2004 to 2019. Adjuvant treatment was classified as HT alone, RT alone, or HT + RT. Male patients were matched with female patients for OS comparison. Survival analysis was performed using Cox regression and Kaplan − Meier method. Inverse probability of treatment weighting (IPTW) was applied to adjust for confounding.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>A total of 523 patients met the inclusion criteria, with 24.4% receiving HT, 16.3% receiving RT, and 59.2% receiving HT + RT. The median follow-up was 6.9 years (IQR: 5.0–9.4 years). IPTW-adjusted 5-yr OS rates in the HT, RT, and HT + RT cohorts were 84.0% (95% CI 77.1–91.5%), 81.1% (95% CI 71.1–92.5%), and 93.0% (95% CI 90.0–96.2%), respectively. On IPTW-adjusted MVA, relative to HT, receipt of HT + RT was associated with improvements in OS (HR: 0.641; <i>p</i> = 0.042). RT alone was not associated with improved OS (HR: 1.264; <i>p</i> = 0.420).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Among men ≥ 65 years old with T1-2N0 HR + breast cancer, RT alone did not confer an OS benefit over HT alone. Combination of RT + HT demonstrated significant improvements in OS. De-escalation of treatment through omission of either RT or HT at this point should be done with caution.</p>","PeriodicalId":56083,"journal":{"name":"Breast Cancer","volume":null,"pages":null},"PeriodicalIF":4.0000,"publicationDate":"2024-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12282-024-01560-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
Randomized clinical trials demonstrate that lumpectomy + hormone therapy (HT) without radiation therapy (RT) yields equivalent survival and acceptable local–regional outcomes in elderly women with early-stage, node-negative, hormone-receptor positive (HR +) breast cancer. Whether these data apply to men with the same inclusion criteria remains unknown.
Methods
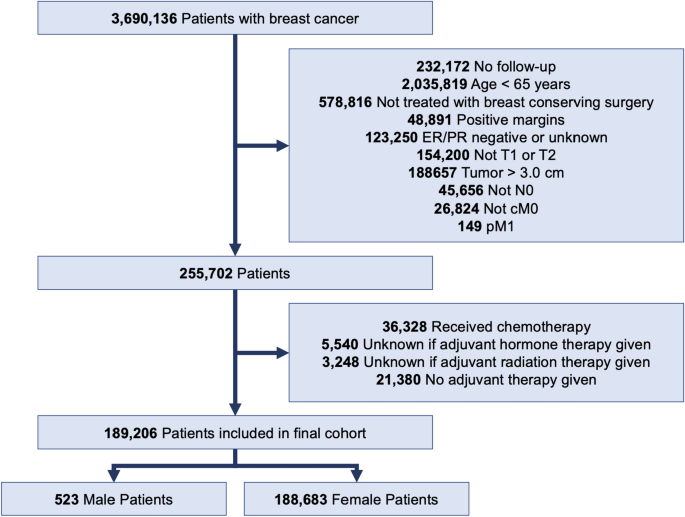
The National Cancer Database was queried for male patients ≥ 65 years with pathologic T1-2N0 (≤ 3 cm) HR + breast cancer treated with breast-conserving surgery with negative margins from 2004 to 2019. Adjuvant treatment was classified as HT alone, RT alone, or HT + RT. Male patients were matched with female patients for OS comparison. Survival analysis was performed using Cox regression and Kaplan − Meier method. Inverse probability of treatment weighting (IPTW) was applied to adjust for confounding.
Results
A total of 523 patients met the inclusion criteria, with 24.4% receiving HT, 16.3% receiving RT, and 59.2% receiving HT + RT. The median follow-up was 6.9 years (IQR: 5.0–9.4 years). IPTW-adjusted 5-yr OS rates in the HT, RT, and HT + RT cohorts were 84.0% (95% CI 77.1–91.5%), 81.1% (95% CI 71.1–92.5%), and 93.0% (95% CI 90.0–96.2%), respectively. On IPTW-adjusted MVA, relative to HT, receipt of HT + RT was associated with improvements in OS (HR: 0.641; p = 0.042). RT alone was not associated with improved OS (HR: 1.264; p = 0.420).
Conclusion
Among men ≥ 65 years old with T1-2N0 HR + breast cancer, RT alone did not confer an OS benefit over HT alone. Combination of RT + HT demonstrated significant improvements in OS. De-escalation of treatment through omission of either RT or HT at this point should be done with caution.
期刊介绍:
Breast Cancer, the official journal of the Japanese Breast Cancer Society, publishes articles that contribute to progress in the field, in basic or translational research and also in clinical research, seeking to develop a new focus and new perspectives for all who are concerned with breast cancer. The journal welcomes all original articles describing clinical and epidemiological studies and laboratory investigations regarding breast cancer and related diseases. The journal will consider five types of articles: editorials, review articles, original articles, case reports, and rapid communications. Although editorials and review articles will principally be solicited by the editors, they can also be submitted for peer review, as in the case of original articles. The journal provides the best of up-to-date information on breast cancer, presenting readers with high-impact, original work focusing on pivotal issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


