Minimally Invasive Correction of Failed Percutaneous Atrial Septal Closure with Device Embolization.
IF 0.3
Q4 SURGERY
Thoracic and Cardiovascular Surgeon Reports
Pub Date : 2024-03-15
eCollection Date: 2024-01-01
DOI:10.1055/a-2276-9898
引用次数: 0
Abstract
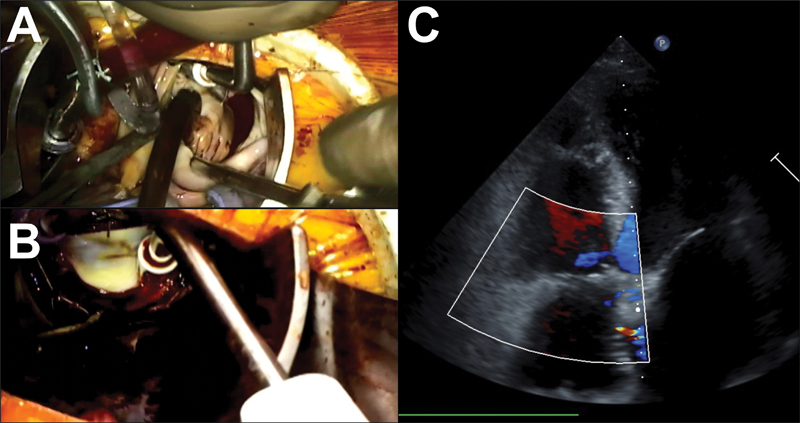
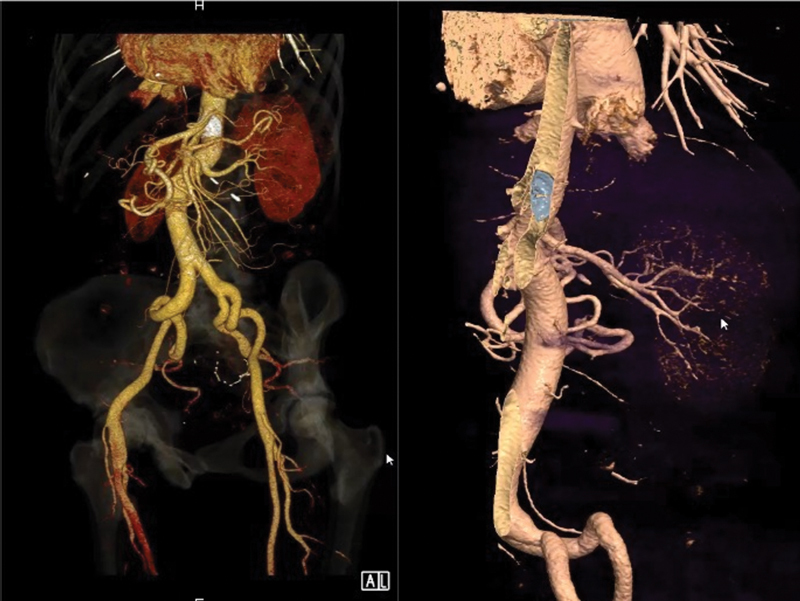
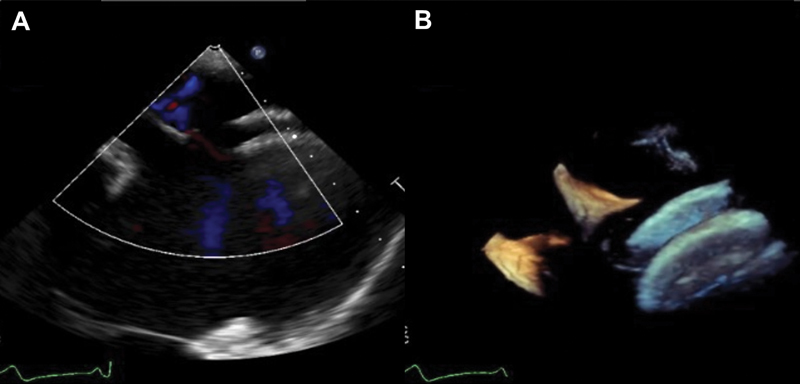
We present the case of a minimally invasive surgical correction for failed percutaneous atrial septal defect (ASD) closure in a 57-year-old female patient with residual ASD, tricuspid regurgitation, atrial fibrillation, and embolization of one of two occluders to the superior mesenteric artery. Our surgical approach consisted of anterolateral minithoracotomy, aortic and femoral vein cannulation, cryoablation, cardiac device removal, closure of ASD with autologous pericardium, and tricuspid repair. The procedure was uneventful and patient was discharged home on postoperative day 4.
通过设备栓塞微创矫正失败的经皮心房隔膜封堵术
我们介绍了一例经皮房间隔缺损(ASD)关闭术失败的微创手术矫正病例,患者是一名 57 岁的女性,伴有 ASD 残留、三尖瓣反流、心房颤动以及肠系膜上动脉两个闭塞器中的一个被栓塞。我们的手术方法包括前外侧小胸廓切开术、主动脉和股静脉插管、低温消融、心脏装置移除、用自体心包封闭 ASD 以及三尖瓣修复。手术过程顺利,患者在术后第 4 天出院回家。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


