{"title":"Efficacy of off-the-shelf bone marrow mesenchymal stem cells for pediatric steroid-refractory acute graft-versus-host disease.","authors":"Hirohito Kubota, Yuki Arakawa, Yoshitaka Mizushima, Tomoya Irikura, Mai Watakabe, Takahiro Ishikawa, Ryota Kaneko, Mamoru Honda, Yuichi Mitani, Kohei Fukuoka, Makiko Mori, Koichi Oshima, Katsuyoshi Koh","doi":"10.31547/bct-2023-020","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Temcell is a mesenchymal stem cell (MSC) product approved for steroid-refractory acute graft-versus-host disease (SR-aGVHD) in Japan. However, reports regarding Temcell's efficacy in pediatric patients have been scarce, and the appropriate use of MSC therapy against pediatric SR-aGVHD also remains to be determined.</p><p><strong>Patients and methods: </strong>We retrospectively assessed a cohort of pediatric patients treated with Temcell for SR-aGVHD following allogeneic hematopoietic transplantation. MSCs were infused intravenously at a dose of 2 × 10<sup>6</sup> cells/kg according to the manufacturer's instructions.</p><p><strong>Results: </strong>Twelve patients received eighteen cycles of MSC therapy (median age, 10.3 [1.7-17.8] years), with four receiving additional cycles (one cycle: n = 3, three cycles: n = 1). The severity of aGVHD before MSC therapy was grade I-II in three patients and grade III-IV in nine patients (gut stage 3-4, n= 7; liver stage 3-4; n =2). The median number of immunosuppressive therapy regimens received prior to MSC administration was two (range: 1-5). The first MSC cycle displayed the best overall response rate of 83%, including six patients with a complete response (CR) and with a 49% reduction in the mean daily dose of prednisone after eight weeks. The median time to first response was 3.5 days (range: 2-15 days). Two of the four patients who were re-administered MSCs for recurrent or persistent GVHD achieved a CR. The three-year overall survival rate was 69.4%, while the three-year failure free survival (FFS) rate was 22.2%, with a median FFS of 4.9 months. There were no observable side effects of MSC therapy.</p><p><strong>Conclusions: </strong>MSC therapy appears to be an effective and safe treatment for pediatric SR-aGVHD, with a steroid-sparing effect and satisfactory efficacy upon re-administration. Further studies are needed to determine its appropriate combination with additional treatments and the optimal use of re-administration of MSCs.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"7 1","pages":"1-9"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10937086/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2023-020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Temcell is a mesenchymal stem cell (MSC) product approved for steroid-refractory acute graft-versus-host disease (SR-aGVHD) in Japan. However, reports regarding Temcell's efficacy in pediatric patients have been scarce, and the appropriate use of MSC therapy against pediatric SR-aGVHD also remains to be determined.
Patients and methods: We retrospectively assessed a cohort of pediatric patients treated with Temcell for SR-aGVHD following allogeneic hematopoietic transplantation. MSCs were infused intravenously at a dose of 2 × 106 cells/kg according to the manufacturer's instructions.
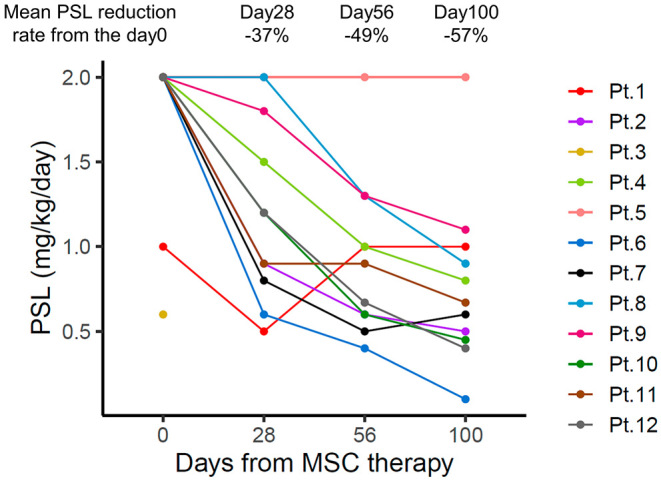
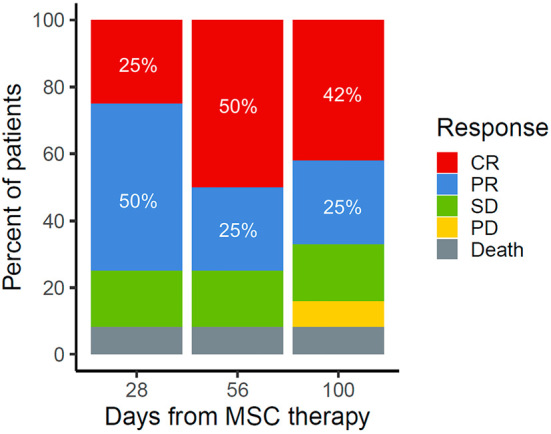
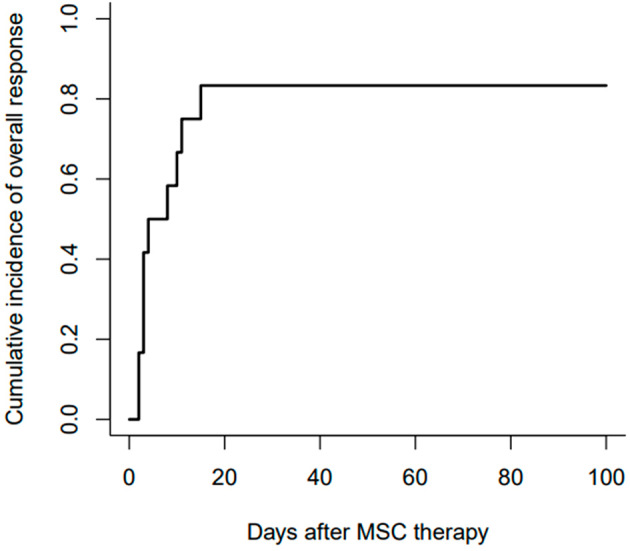
Results: Twelve patients received eighteen cycles of MSC therapy (median age, 10.3 [1.7-17.8] years), with four receiving additional cycles (one cycle: n = 3, three cycles: n = 1). The severity of aGVHD before MSC therapy was grade I-II in three patients and grade III-IV in nine patients (gut stage 3-4, n= 7; liver stage 3-4; n =2). The median number of immunosuppressive therapy regimens received prior to MSC administration was two (range: 1-5). The first MSC cycle displayed the best overall response rate of 83%, including six patients with a complete response (CR) and with a 49% reduction in the mean daily dose of prednisone after eight weeks. The median time to first response was 3.5 days (range: 2-15 days). Two of the four patients who were re-administered MSCs for recurrent or persistent GVHD achieved a CR. The three-year overall survival rate was 69.4%, while the three-year failure free survival (FFS) rate was 22.2%, with a median FFS of 4.9 months. There were no observable side effects of MSC therapy.
Conclusions: MSC therapy appears to be an effective and safe treatment for pediatric SR-aGVHD, with a steroid-sparing effect and satisfactory efficacy upon re-administration. Further studies are needed to determine its appropriate combination with additional treatments and the optimal use of re-administration of MSCs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


