Splenic injury caused by cardiopulmonary resuscitation in a full stomach with hematoma after hemorrhagic shock due to bleeding duodenal ulcer: A case report
{"title":"Splenic injury caused by cardiopulmonary resuscitation in a full stomach with hematoma after hemorrhagic shock due to bleeding duodenal ulcer: A case report","authors":"Daisuke Fujimori, Tomohide Koyama, Satomi Ooki, Masaaki Ito, Yasutaka Yoshiike, Satoshi Nakamura, Ryuhei Yoshida, So Sakamoto, Chikao Ito, Miyuki Kasuya, Kyoji Oe, Isao Takahashi","doi":"10.1002/ams2.940","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Cardiopulmonary resuscitation is essential for cardiopulmonary arrest, but complications from chest compressions warrant monitoring. Although rib and sternal fractures are common, abdominal injuries are rare, and splenic injuries are much rarer.</p>\n </section>\n \n <section>\n \n <h3> Case Presentation</h3>\n \n <p>A 74-year-old man was admitted to the emergency room with a hemorrhagic duodenal ulcer. During hospitalization, the patient went into cardiopulmonary arrest due to hemorrhagic shock. Spontaneous circulation returned after 7 min of cardiopulmonary resuscitation. He underwent transcatheter arterial embolization to stop the bleeding from the duodenal ulcer. The next day, a close examination of the patient's progressive anemia revealed splenic injury; transcatheter arterial embolization was performed to save his life.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>It is important to consider the complication of splenic injury in patients with cardiopulmonary arrest who have undergone appropriate cardiopulmonary resuscitation. A possible mechanism—especially in patients with a full stomach—is the squeezing of the spleen by the diaphragm, abdominal wall, and stomach.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.940","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.940","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Cardiopulmonary resuscitation is essential for cardiopulmonary arrest, but complications from chest compressions warrant monitoring. Although rib and sternal fractures are common, abdominal injuries are rare, and splenic injuries are much rarer.
Case Presentation
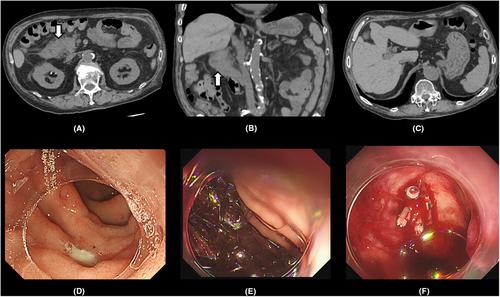
A 74-year-old man was admitted to the emergency room with a hemorrhagic duodenal ulcer. During hospitalization, the patient went into cardiopulmonary arrest due to hemorrhagic shock. Spontaneous circulation returned after 7 min of cardiopulmonary resuscitation. He underwent transcatheter arterial embolization to stop the bleeding from the duodenal ulcer. The next day, a close examination of the patient's progressive anemia revealed splenic injury; transcatheter arterial embolization was performed to save his life.
Conclusion
It is important to consider the complication of splenic injury in patients with cardiopulmonary arrest who have undergone appropriate cardiopulmonary resuscitation. A possible mechanism—especially in patients with a full stomach—is the squeezing of the spleen by the diaphragm, abdominal wall, and stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


