Comparative evaluation of continuous infusion versus programmed intermittent bolus techniques in erector spinae plane block in modified radical mastectomy - A preliminary randomised controlled trial.
Thamizharasan Datchinamourthy, Debesh Bhoi, Anjolie Chhabra, Virender K Mohan, Kanil R Kumar, Poornima Ranganathan
{"title":"Comparative evaluation of continuous infusion versus programmed intermittent bolus techniques in erector spinae plane block in modified radical mastectomy - A preliminary randomised controlled trial.","authors":"Thamizharasan Datchinamourthy, Debesh Bhoi, Anjolie Chhabra, Virender K Mohan, Kanil R Kumar, Poornima Ranganathan","doi":"10.4103/ija.ija_922_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Single-shot erector spinae plane block (ESPB) provides excellent analgesia in mastectomy in the immediate post-operative period but is not sufficient to maintain for prolonged duration. This study compares the efficacy of programmed intermittent bolus (PIB) versus continuous infusion (CI) techniques after ESPB by placing a catheter for mastectomy.</p><p><strong>Methods: </strong>After ethical approval and patient consent, ESPB was performed at the T4 level in 50 patients with an initial bolus of 20 mL 0.375% ropivacaine and a catheter placed 30 min before surgery. In the postoperative period, they were randomised to Group I - intermittent bolus of 20 mL 0.2% ropivacaine every 4 h for 24 h and Group C - continuous infusion of 0.2% ropivacaine at 5 mL/h for 24 h. The primary outcome was the 24-h fentanyl consumption by patient-controlled analgesia device. Data was analysed using Stata 14.0.</p><p><strong>Results: </strong>Group I patients had reduced post-operative fentanyl consumption {mean [standard deviation (SD)]: 166 (139.17) µg vs 332 (247.96) µg, <i>P</i> = 0.002} and lower median NRS scores (1 h: 3 vs 5), (2 h: 3 vs 5), (4 h: 3 vs 5), (6 h: 4 vs 5) with a higher mean (SD) Quality of Recovery-15 score {134.4 (8.53) vs 127 (12.89), <i>P</i> = 0.020} compared to Group C, respectively. The 24-h dermatomal sensory coverage was more comprehensive in Group I compared to Group C.</p><p><strong>Conclusion: </strong>The PIB technique after ESPB provides decreased postoperative opioid consumption, better post-operative analgesia and quality of recovery compared to the CI technique in patients undergoing mastectomy.</p>","PeriodicalId":13339,"journal":{"name":"Indian Journal of Anaesthesia","volume":"68 3","pages":"273-279"},"PeriodicalIF":1.9000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10926334/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ija.ija_922_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Single-shot erector spinae plane block (ESPB) provides excellent analgesia in mastectomy in the immediate post-operative period but is not sufficient to maintain for prolonged duration. This study compares the efficacy of programmed intermittent bolus (PIB) versus continuous infusion (CI) techniques after ESPB by placing a catheter for mastectomy.
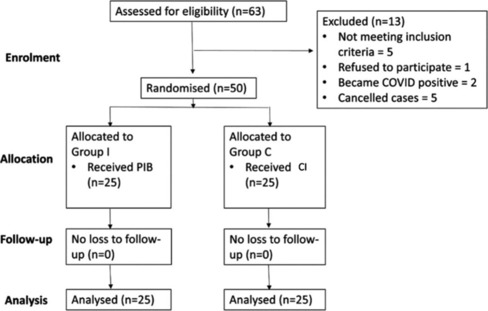
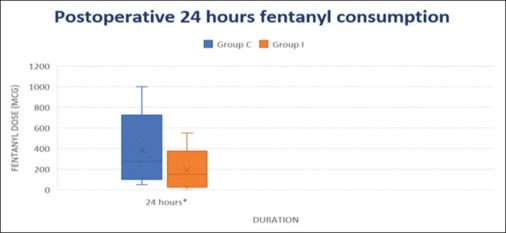
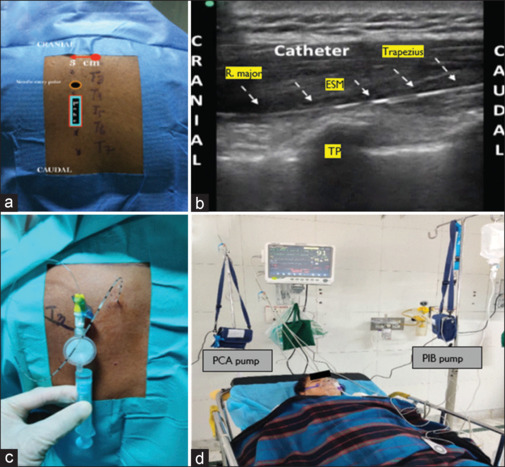
Methods: After ethical approval and patient consent, ESPB was performed at the T4 level in 50 patients with an initial bolus of 20 mL 0.375% ropivacaine and a catheter placed 30 min before surgery. In the postoperative period, they were randomised to Group I - intermittent bolus of 20 mL 0.2% ropivacaine every 4 h for 24 h and Group C - continuous infusion of 0.2% ropivacaine at 5 mL/h for 24 h. The primary outcome was the 24-h fentanyl consumption by patient-controlled analgesia device. Data was analysed using Stata 14.0.
Results: Group I patients had reduced post-operative fentanyl consumption {mean [standard deviation (SD)]: 166 (139.17) µg vs 332 (247.96) µg, P = 0.002} and lower median NRS scores (1 h: 3 vs 5), (2 h: 3 vs 5), (4 h: 3 vs 5), (6 h: 4 vs 5) with a higher mean (SD) Quality of Recovery-15 score {134.4 (8.53) vs 127 (12.89), P = 0.020} compared to Group C, respectively. The 24-h dermatomal sensory coverage was more comprehensive in Group I compared to Group C.
Conclusion: The PIB technique after ESPB provides decreased postoperative opioid consumption, better post-operative analgesia and quality of recovery compared to the CI technique in patients undergoing mastectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


