Simon Sensalire, Abel Nkolo, Juliana Nabwire Ssali, Martin Muhire, Augustin Muhwezi, Herbert Kadama
{"title":"Applying a Three-Tier Approach to Address Gaps in Oral Pre-Exposure Prophylaxis Uptake and Continuity in Uganda: A Mixed Methods Approach.","authors":"Simon Sensalire, Abel Nkolo, Juliana Nabwire Ssali, Martin Muhire, Augustin Muhwezi, Herbert Kadama","doi":"10.9745/GHSP-D-23-00229","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We describe a 3-tier approach involving a gap analysis, root cause analysis, and pre-exposure prophylaxis (PrEP) collaborative to understand the gap and identify and address the main barriers to oral PrEP uptake and continuity in Uganda.</p><p><strong>Methods: </strong>We used a mixed methods design with retrospective, cross-sectional, and prospective components. The gap analysis involved descriptive analysis of PrEP uptake and continuity. The RCA identified the main barriers to initiation and continuity on PrEP among 1,334 clients who declined to start PrEP and 1,266 who missed their appointment but were at risk. The PrEP collaborative tested changes mapped onto specific barriers to optimize the PrEP clinical service delivery. A trend analysis of routinely collected data of the PrEP cascade determined significant shifts and trends in PrEP uptake and continuity.</p><p><strong>Results: </strong>Only 60% of the high-risk population eligible for PrEP were enrolled, while fewer than 30% of the cumulative number of PrEP users were refilled each quarter. Uncertainty and fear of side effects, perceptions about the harmfulness of the medication, perceived inability to adhere to PrEP, and stigma were the main reasons why clients rejected PrEP. Lack of access to the facility, side effects, pill burden, stigma, perceived low-risk exposure to HIV, and preference of staying at work as opposed to picking up refills affected continuity on PrEP. The collaborative registered statistically significant shifts in PrEP enrollment from 64% to 89% and continuity from 51% to 78% between July 21 and November 22 following the collaborative intervention.</p><p><strong>Conclusions: </strong>We recommend using a 3-tier approach for other similar implementation contexts to strengthen PrEP programming, given the marked statistical shift in PrEP uptake and continuity. This begins with understanding the gap and barriers to use among clients, followed by mapping interventions to specific barriers through a quality improvement collaborative.</p>","PeriodicalId":12692,"journal":{"name":"Global Health: Science and Practice","volume":" ","pages":""},"PeriodicalIF":2.5000,"publicationDate":"2024-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11057795/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health: Science and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.9745/GHSP-D-23-00229","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
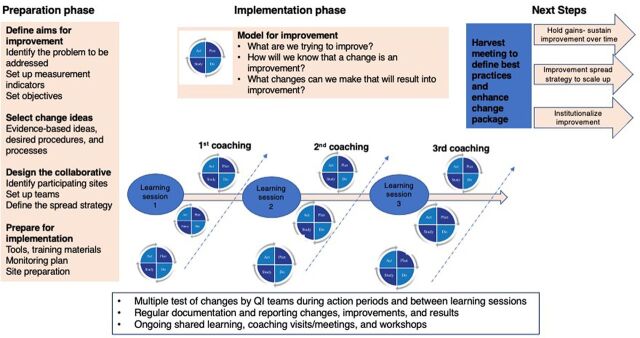
Background: We describe a 3-tier approach involving a gap analysis, root cause analysis, and pre-exposure prophylaxis (PrEP) collaborative to understand the gap and identify and address the main barriers to oral PrEP uptake and continuity in Uganda.
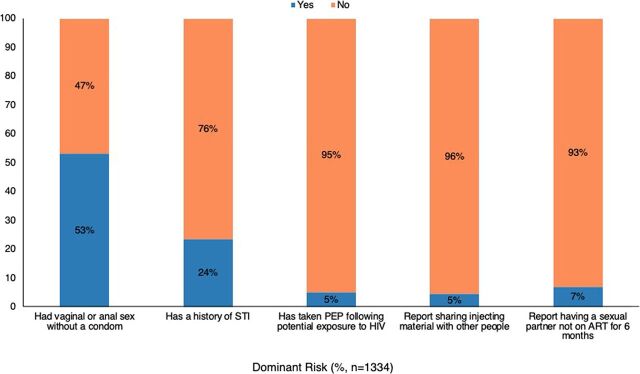
Methods: We used a mixed methods design with retrospective, cross-sectional, and prospective components. The gap analysis involved descriptive analysis of PrEP uptake and continuity. The RCA identified the main barriers to initiation and continuity on PrEP among 1,334 clients who declined to start PrEP and 1,266 who missed their appointment but were at risk. The PrEP collaborative tested changes mapped onto specific barriers to optimize the PrEP clinical service delivery. A trend analysis of routinely collected data of the PrEP cascade determined significant shifts and trends in PrEP uptake and continuity.
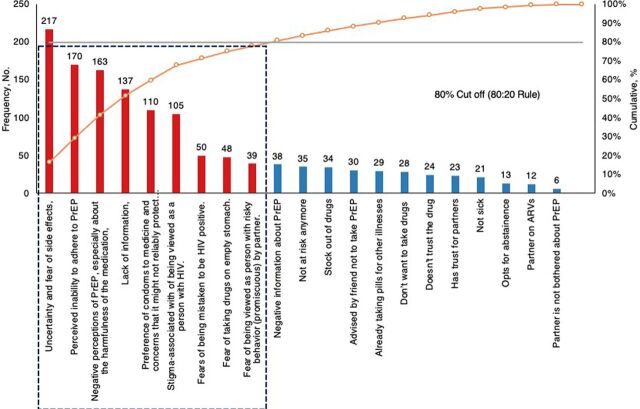
Results: Only 60% of the high-risk population eligible for PrEP were enrolled, while fewer than 30% of the cumulative number of PrEP users were refilled each quarter. Uncertainty and fear of side effects, perceptions about the harmfulness of the medication, perceived inability to adhere to PrEP, and stigma were the main reasons why clients rejected PrEP. Lack of access to the facility, side effects, pill burden, stigma, perceived low-risk exposure to HIV, and preference of staying at work as opposed to picking up refills affected continuity on PrEP. The collaborative registered statistically significant shifts in PrEP enrollment from 64% to 89% and continuity from 51% to 78% between July 21 and November 22 following the collaborative intervention.
Conclusions: We recommend using a 3-tier approach for other similar implementation contexts to strengthen PrEP programming, given the marked statistical shift in PrEP uptake and continuity. This begins with understanding the gap and barriers to use among clients, followed by mapping interventions to specific barriers through a quality improvement collaborative.
期刊介绍:
Global Health: Science and Practice (GHSP) is a no-fee, open-access, peer-reviewed, online journal aimed to improve health practice, especially in low- and middle-income countries. Our goal is to reach those who design, implement, manage, evaluate, and otherwise support health programs. We are especially interested in advancing knowledge on practical program implementation issues, with information on what programs entail and how they are implemented. GHSP is currently indexed in PubMed, PubMed Central, POPLINE, EBSCO, SCOPUS,. the Web of Science Emerging Sources Citation Index, and the USAID Development Experience Clearinghouse (DEC).
TOPICS:
Issued four times a year, GHSP will include articles on all global health topics, covering diverse programming models and a wide range of cross-cutting issues that impact and support health systems. Examples include but are not limited to:
Health:
Addiction and harm reduction,
Child Health,
Communicable and Emerging Diseases,
Disaster Preparedness and Response,
Environmental Health,
Family Planning/Reproductive Health,
HIV/AIDS,
Malaria,
Maternal Health,
Neglected Tropical Diseases,
Non-Communicable Diseases/Injuries,
Nutrition,
Tuberculosis,
Water and Sanitation.
Cross-Cutting Issues:
Epidemiology,
Gender,
Health Communication/Healthy Behavior,
Health Policy and Advocacy,
Health Systems,
Human Resources/Training,
Knowledge Management,
Logistics and Supply Chain Management,
Management and Governance,
mHealth/eHealth/digital health,
Monitoring and Evaluation,
Scale Up,
Youth.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


