Roger G. Evans, Andrew D. Cochrane, Sally G. Hood, Bruno Marino, Naoya Iguchi, Rinaldo Bellomo, Peter R. McCall, Nobuki Okazaki, Alemayehu H. Jufar, Lachlan F. Miles, Taku Furukawa, Connie P. C. Ow, Jaishankar Raman, Clive N. May, Yugeesh R. Lankadeva
{"title":"Differential responses of cerebral and renal oxygenation to altered perfusion conditions during experimental cardiopulmonary bypass in sheep","authors":"Roger G. Evans, Andrew D. Cochrane, Sally G. Hood, Bruno Marino, Naoya Iguchi, Rinaldo Bellomo, Peter R. McCall, Nobuki Okazaki, Alemayehu H. Jufar, Lachlan F. Miles, Taku Furukawa, Connie P. C. Ow, Jaishankar Raman, Clive N. May, Yugeesh R. Lankadeva","doi":"10.1111/1440-1681.13852","DOIUrl":null,"url":null,"abstract":"<p>We tested whether the brain and kidney respond differently to cardiopulmonary bypass (CPB) and to changes in perfusion conditions during CPB. Therefore, in ovine CPB, we assessed regional cerebral oxygen saturation (rSO<sub>2</sub>) by near-infrared spectroscopy and renal cortical and medullary tissue oxygen tension (PO<sub>2</sub>), and, in some protocols, brain tissue PO<sub>2</sub>, by phosphorescence lifetime oximetry. During CPB, rSO<sub>2</sub> correlated with mixed venous SO<sub>2</sub> (r = 0.78) and brain tissue PO<sub>2</sub> (r = 0.49) when arterial PO<sub>2</sub> was varied. During the first 30 min of CPB, brain tissue PO<sub>2</sub>, rSO<sub>2</sub> and renal cortical tissue PO<sub>2</sub> did not fall, but renal medullary tissue PO<sub>2</sub> did. Nevertheless, compared with stable anaesthesia, during stable CPB, rSO<sub>2</sub> (66.8 decreasing to 61.3%) and both renal cortical (90.8 decreasing to 43.5 mm Hg) and medullary (44.3 decreasing to 19.2 mm Hg) tissue PO<sub>2</sub> were lower. Both rSO<sub>2</sub> and renal PO<sub>2</sub> increased when pump flow was increased from 60 to 100 mL kg<sup>−1</sup> min<sup>−1</sup> at a target arterial pressure of 70 mm Hg. They also both increased when pump flow and arterial pressure were increased simultaneously. Neither was significantly altered by partially pulsatile flow. The vasopressor, metaraminol, dose-dependently decreased rSO<sub>2</sub>, but increased renal cortical and medullary PO<sub>2</sub>. Increasing blood haemoglobin concentration increased rSO<sub>2</sub>, but not renal PO<sub>2</sub>. We conclude that both the brain and kidney are susceptible to hypoxia during CPB, which can be alleviated by increasing pump flow, even without increasing arterial pressure. However, increasing blood haemoglobin concentration increases brain, but not kidney oxygenation, whereas vasopressor support with metaraminol increases kidney, but not brain oxygenation.</p>","PeriodicalId":50684,"journal":{"name":"Clinical and Experimental Pharmacology and Physiology","volume":"51 4","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1440-1681.13852","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Pharmacology and Physiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1440-1681.13852","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
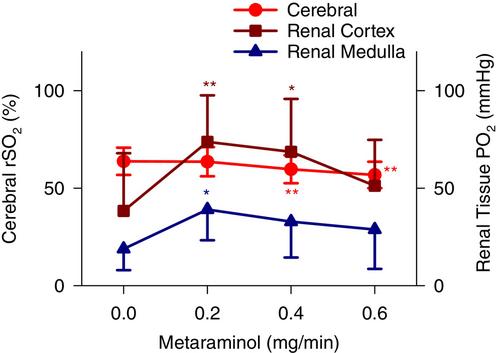
We tested whether the brain and kidney respond differently to cardiopulmonary bypass (CPB) and to changes in perfusion conditions during CPB. Therefore, in ovine CPB, we assessed regional cerebral oxygen saturation (rSO2) by near-infrared spectroscopy and renal cortical and medullary tissue oxygen tension (PO2), and, in some protocols, brain tissue PO2, by phosphorescence lifetime oximetry. During CPB, rSO2 correlated with mixed venous SO2 (r = 0.78) and brain tissue PO2 (r = 0.49) when arterial PO2 was varied. During the first 30 min of CPB, brain tissue PO2, rSO2 and renal cortical tissue PO2 did not fall, but renal medullary tissue PO2 did. Nevertheless, compared with stable anaesthesia, during stable CPB, rSO2 (66.8 decreasing to 61.3%) and both renal cortical (90.8 decreasing to 43.5 mm Hg) and medullary (44.3 decreasing to 19.2 mm Hg) tissue PO2 were lower. Both rSO2 and renal PO2 increased when pump flow was increased from 60 to 100 mL kg−1 min−1 at a target arterial pressure of 70 mm Hg. They also both increased when pump flow and arterial pressure were increased simultaneously. Neither was significantly altered by partially pulsatile flow. The vasopressor, metaraminol, dose-dependently decreased rSO2, but increased renal cortical and medullary PO2. Increasing blood haemoglobin concentration increased rSO2, but not renal PO2. We conclude that both the brain and kidney are susceptible to hypoxia during CPB, which can be alleviated by increasing pump flow, even without increasing arterial pressure. However, increasing blood haemoglobin concentration increases brain, but not kidney oxygenation, whereas vasopressor support with metaraminol increases kidney, but not brain oxygenation.
期刊介绍:
Clinical and Experimental Pharmacology and Physiology is an international journal founded in 1974 by Mike Rand, Austin Doyle, John Coghlan and Paul Korner. Our focus is new frontiers in physiology and pharmacology, emphasizing the translation of basic research to clinical practice. We publish original articles, invited reviews and our exciting, cutting-edge Frontiers-in-Research series’.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


