Electroencephalographic guided propofol-remifentanil TCI anesthesia with and without dexmedetomidine in a geriatric population: electroencephalographic signatures and clinical evaluation.
Dominik M Mehler, Matthias Kreuzer, David P Obert, Luis F Cardenas, Ignacio Barra, Fernando Zurita, Francisco A Lobo, Stephan Kratzer, Gerhard Schneider, Pablo O Sepúlveda
{"title":"Electroencephalographic guided propofol-remifentanil TCI anesthesia with and without dexmedetomidine in a geriatric population: electroencephalographic signatures and clinical evaluation.","authors":"Dominik M Mehler, Matthias Kreuzer, David P Obert, Luis F Cardenas, Ignacio Barra, Fernando Zurita, Francisco A Lobo, Stephan Kratzer, Gerhard Schneider, Pablo O Sepúlveda","doi":"10.1007/s10877-024-01127-4","DOIUrl":null,"url":null,"abstract":"<p><p>Elderly and multimorbid patients are at high risk for developing unfavorable postoperative neurocognitive outcomes; however, well-adjusted and EEG-guided anesthesia may help titrate anesthesia and improve postoperative outcomes. Over the last decade, dexmedetomidine has been increasingly used as an adjunct in the perioperative setting. Its synergistic effect with propofol decreases the dose of propofol needed to induce and maintain general anesthesia. In this pilot study, we evaluate two highly standardized anesthetic regimens for their potential to prevent burst suppression and postoperative neurocognitive dysfunction in a high-risk population. Prospective, randomized clinical trial with non-blinded intervention. Operating room and post anesthesia care unit at Hospital Base San José, Osorno/Universidad Austral, Valdivia, Chile. 23 patients with scheduled non-neurologic, non-cardiac surgeries with age > 69 years and a planned intervention time > 60 min. Patients were randomly assigned to receive either a propofol-remifentanil based anesthesia or an anesthetic regimen with dexmedetomidine-propofol-remifentanil. All patients underwent a slow titrated induction, followed by a target controlled infusion (TCI) of propofol and remifentanil (n = 10) or propofol, remifentanil and continuous dexmedetomidine infusion (n = 13). We compared the perioperative EEG signatures, drug-induced changes, and neurocognitive outcomes between two anesthetic regimens in geriatric patients. We conducted a pre- and postoperative Montreal Cognitive Assessment (MoCa) test and measured the level of alertness postoperatively using a sedation agitation scale to assess neurocognitive status. During slow induction, maintenance, and emergence, burst suppression was not observed in either group; however, EEG signatures differed significantly between the two groups. In general, EEG activity in the propofol group was dominated by faster rhythms than in the dexmedetomidine group. Time to responsiveness was not significantly different between the two groups (p = 0.352). Finally, no significant differences were found in postoperative cognitive outcomes evaluated by the MoCa test nor sedation agitation scale up to one hour after extubation. This pilot study demonstrates that the two proposed anesthetic regimens can be safely used to slowly induce anesthesia and avoid EEG burst suppression patterns. Despite the patients being elderly and at high risk, we did not observe postoperative neurocognitive deficits. The reduced alpha power in the dexmedetomidine-treated group was not associated with adverse neurocognitive outcomes.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"803-815"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01127-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
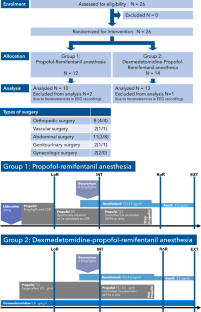
Elderly and multimorbid patients are at high risk for developing unfavorable postoperative neurocognitive outcomes; however, well-adjusted and EEG-guided anesthesia may help titrate anesthesia and improve postoperative outcomes. Over the last decade, dexmedetomidine has been increasingly used as an adjunct in the perioperative setting. Its synergistic effect with propofol decreases the dose of propofol needed to induce and maintain general anesthesia. In this pilot study, we evaluate two highly standardized anesthetic regimens for their potential to prevent burst suppression and postoperative neurocognitive dysfunction in a high-risk population. Prospective, randomized clinical trial with non-blinded intervention. Operating room and post anesthesia care unit at Hospital Base San José, Osorno/Universidad Austral, Valdivia, Chile. 23 patients with scheduled non-neurologic, non-cardiac surgeries with age > 69 years and a planned intervention time > 60 min. Patients were randomly assigned to receive either a propofol-remifentanil based anesthesia or an anesthetic regimen with dexmedetomidine-propofol-remifentanil. All patients underwent a slow titrated induction, followed by a target controlled infusion (TCI) of propofol and remifentanil (n = 10) or propofol, remifentanil and continuous dexmedetomidine infusion (n = 13). We compared the perioperative EEG signatures, drug-induced changes, and neurocognitive outcomes between two anesthetic regimens in geriatric patients. We conducted a pre- and postoperative Montreal Cognitive Assessment (MoCa) test and measured the level of alertness postoperatively using a sedation agitation scale to assess neurocognitive status. During slow induction, maintenance, and emergence, burst suppression was not observed in either group; however, EEG signatures differed significantly between the two groups. In general, EEG activity in the propofol group was dominated by faster rhythms than in the dexmedetomidine group. Time to responsiveness was not significantly different between the two groups (p = 0.352). Finally, no significant differences were found in postoperative cognitive outcomes evaluated by the MoCa test nor sedation agitation scale up to one hour after extubation. This pilot study demonstrates that the two proposed anesthetic regimens can be safely used to slowly induce anesthesia and avoid EEG burst suppression patterns. Despite the patients being elderly and at high risk, we did not observe postoperative neurocognitive deficits. The reduced alpha power in the dexmedetomidine-treated group was not associated with adverse neurocognitive outcomes.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


