Jay K Shah, Laith Z Abwini, Alex Tang, Jason I Yang, David M Keller, Luke G Menken, Frank A Liporace, Richard S Yoon
{"title":"Comparative outcomes after treatment of peri-implant, periprosthetic, and interprosthetic femur fractures: which factors increase mortality risk?","authors":"Jay K Shah, Laith Z Abwini, Alex Tang, Jason I Yang, David M Keller, Luke G Menken, Frank A Liporace, Richard S Yoon","doi":"10.1097/OI9.0000000000000322","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare mortality rates between patients treated surgically for periprosthetic fractures (PPF) after total hip arthroplasty (THA), total knee arthroplasty (TKA), peri-implant (PI), and interprosthetic (IP) fractures while identifying risk factors associated with mortality following PPF.</p><p><strong>Design: </strong>Retrospective.</p><p><strong>Setting: </strong>Single, Level II Trauma Center.</p><p><strong>Patients/participants: </strong>A retrospective review was conducted of 129 consecutive patients treated surgically for fractures around a pre-existing prosthesis or implant from 2013 to 2020. Patients were separated into 4 comparison groups: THA, TKA, PI, and IP fractures.</p><p><strong>Intervention: </strong>Revision implant or arthroplasty, open reduction and internal fixation (ORIF), intramedullary nailing (IMN), percutaneous screws, or a combination of techniques.</p><p><strong>Main outcome measurements: </strong>Primary outcome measures include mortality rates of different types of PPF, PI, and IP fractures at 1-month, 3-month, 6-month, 1-year, and 2-year postoperative. We analyzed risk factors associated with mortality aimed to determine whether treatment type affects mortality.</p><p><strong>Results: </strong>One hundred twenty-nine patients were included for final analysis. Average follow-up was similar between all groups. The overall 1-year mortality rate was 1 month (5%), 3 months (12%), 6 months (13%), 1 year (15%), and 2 years (22%). There were no differences in mortality rates between each group at 30 days, 90 days, 6 months, 1 year, and 2 years (<i>P</i>-value = 0.86). A Kaplan-Meier survival curve demonstrated no difference in survivorship up to 2 years. Older than 65 years, history of hypothyroidism and dementia, and discharge to a skilled nursing facility (SNF) led to increased mortality. There was no survival benefit in treating patients with PPFs with either revision, ORIF, IMN, or a combination of techniques.</p><p><strong>Conclusion: </strong>The overall mortality rates observed were 1 month (5%), 3 months (12%), 6 months (13%), 1 year (15%), and 2 years (22%), and no differences were found between each group at all follow-up time points. Patients aged 65 and older with a history of hypothyroidism and/or dementia discharged to an SNF are at increased risk for mortality. From a mortality perspective, surgeons should not hesitate to choose the surgical treatment they feel most comfortable performing.</p><p><strong>Level of evidence: </strong>Level III.</p>","PeriodicalId":74381,"journal":{"name":"OTA international : the open access journal of orthopaedic trauma","volume":"7 1","pages":"e322"},"PeriodicalIF":0.0000,"publicationDate":"2024-02-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10904097/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTA international : the open access journal of orthopaedic trauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/OI9.0000000000000322","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To compare mortality rates between patients treated surgically for periprosthetic fractures (PPF) after total hip arthroplasty (THA), total knee arthroplasty (TKA), peri-implant (PI), and interprosthetic (IP) fractures while identifying risk factors associated with mortality following PPF.
Design: Retrospective.
Setting: Single, Level II Trauma Center.
Patients/participants: A retrospective review was conducted of 129 consecutive patients treated surgically for fractures around a pre-existing prosthesis or implant from 2013 to 2020. Patients were separated into 4 comparison groups: THA, TKA, PI, and IP fractures.
Intervention: Revision implant or arthroplasty, open reduction and internal fixation (ORIF), intramedullary nailing (IMN), percutaneous screws, or a combination of techniques.
Main outcome measurements: Primary outcome measures include mortality rates of different types of PPF, PI, and IP fractures at 1-month, 3-month, 6-month, 1-year, and 2-year postoperative. We analyzed risk factors associated with mortality aimed to determine whether treatment type affects mortality.
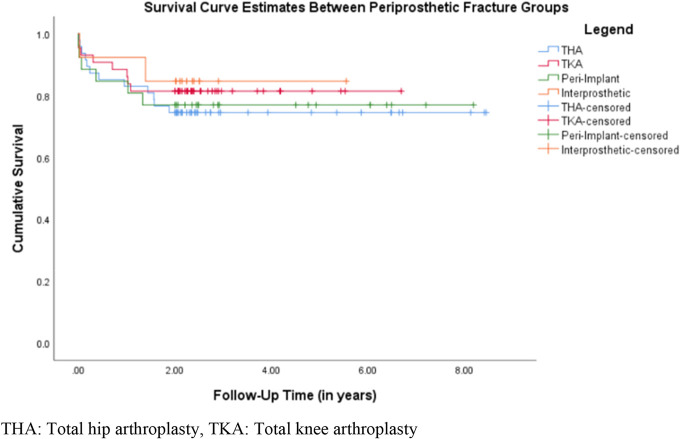
Results: One hundred twenty-nine patients were included for final analysis. Average follow-up was similar between all groups. The overall 1-year mortality rate was 1 month (5%), 3 months (12%), 6 months (13%), 1 year (15%), and 2 years (22%). There were no differences in mortality rates between each group at 30 days, 90 days, 6 months, 1 year, and 2 years (P-value = 0.86). A Kaplan-Meier survival curve demonstrated no difference in survivorship up to 2 years. Older than 65 years, history of hypothyroidism and dementia, and discharge to a skilled nursing facility (SNF) led to increased mortality. There was no survival benefit in treating patients with PPFs with either revision, ORIF, IMN, or a combination of techniques.
Conclusion: The overall mortality rates observed were 1 month (5%), 3 months (12%), 6 months (13%), 1 year (15%), and 2 years (22%), and no differences were found between each group at all follow-up time points. Patients aged 65 and older with a history of hypothyroidism and/or dementia discharged to an SNF are at increased risk for mortality. From a mortality perspective, surgeons should not hesitate to choose the surgical treatment they feel most comfortable performing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


