Cedric Lau, Ma Ida Mohmaed Ali, Lishi Lin, Dorieke E M van Balen, Bart A W Jacobs, Bastiaan Nuijen, Robert M Smeenk, Neeltje Steeghs, Alwin D R Huitema
{"title":"Impact of bariatric surgery on oral anticancer drugs: an analysis of real-world data.","authors":"Cedric Lau, Ma Ida Mohmaed Ali, Lishi Lin, Dorieke E M van Balen, Bart A W Jacobs, Bastiaan Nuijen, Robert M Smeenk, Neeltje Steeghs, Alwin D R Huitema","doi":"10.1007/s00280-024-04640-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The number of patients with bariatric surgery who receive oral anticancer drugs is rising. Bariatric surgery may affect the absorption of oral anticancer drugs. Strikingly, no specific drug dosing recommendations are available. We aim to provide practical recommendations on the application of oral anticancer drugs in patients who underwent bariatric surgery.</p><p><strong>Methods: </strong>Patients with any kind of bariatric surgery were extracted retrospectively in a comprehensive cancer center. In addition, a flowchart was proposed to assess the risk of inadequate exposure to oral anticancer drugs in patients who underwent bariatric surgery. Subsequently, the flowchart was evaluated retrospectively using routine Therapeutic drug monitoring (TDM) samples.</p><p><strong>Results: </strong>In our analysis, 571 cancer patients (0.4% of 140.000 treated or referred patients) had previous bariatric surgery. Of these patients, 78 unique patients received 152 oral anticancer drugs equaling an overall number of 30 unique drugs. The 30 different prescribed oral anticancer drugs were categorized as low risk (13%), medium risk (67%), and high risk (20%) of underdosing. TDM plasma samples of 25 patients (82 samples) were available, of which 21 samples post-bariatric surgery (25%) were below the target value.</p><p><strong>Conclusions: </strong>The proposed flowchart can support optimizing the treatment with orally administered anticancer drugs in patients who underwent bariatric surgery. We recommend performing TDM in drugs that belong to BCS classes II, III, or IV. If more risk factors are present in BCS classes II or IV, a priori switches to other drugs may be advised. In specific cases, higher dosages can be provided from the start (e.g., tamoxifen).</p>","PeriodicalId":9556,"journal":{"name":"Cancer Chemotherapy and Pharmacology","volume":" ","pages":"25-34"},"PeriodicalIF":2.7000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11258081/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Chemotherapy and Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00280-024-04640-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The number of patients with bariatric surgery who receive oral anticancer drugs is rising. Bariatric surgery may affect the absorption of oral anticancer drugs. Strikingly, no specific drug dosing recommendations are available. We aim to provide practical recommendations on the application of oral anticancer drugs in patients who underwent bariatric surgery.
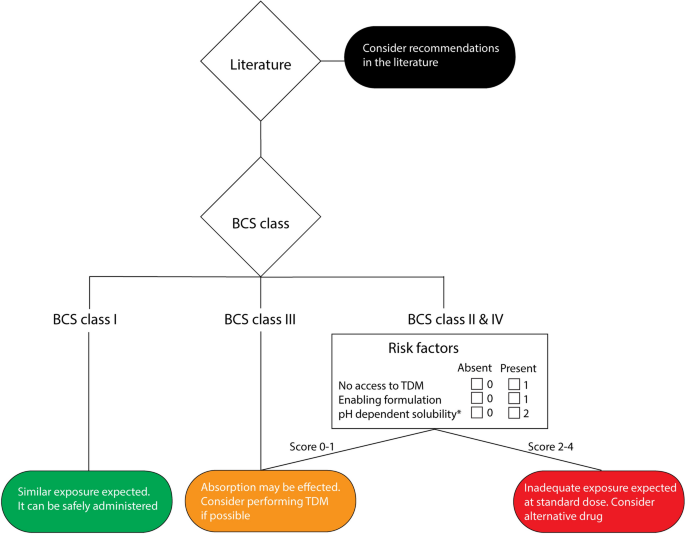
Methods: Patients with any kind of bariatric surgery were extracted retrospectively in a comprehensive cancer center. In addition, a flowchart was proposed to assess the risk of inadequate exposure to oral anticancer drugs in patients who underwent bariatric surgery. Subsequently, the flowchart was evaluated retrospectively using routine Therapeutic drug monitoring (TDM) samples.
Results: In our analysis, 571 cancer patients (0.4% of 140.000 treated or referred patients) had previous bariatric surgery. Of these patients, 78 unique patients received 152 oral anticancer drugs equaling an overall number of 30 unique drugs. The 30 different prescribed oral anticancer drugs were categorized as low risk (13%), medium risk (67%), and high risk (20%) of underdosing. TDM plasma samples of 25 patients (82 samples) were available, of which 21 samples post-bariatric surgery (25%) were below the target value.
Conclusions: The proposed flowchart can support optimizing the treatment with orally administered anticancer drugs in patients who underwent bariatric surgery. We recommend performing TDM in drugs that belong to BCS classes II, III, or IV. If more risk factors are present in BCS classes II or IV, a priori switches to other drugs may be advised. In specific cases, higher dosages can be provided from the start (e.g., tamoxifen).
期刊介绍:
Addressing a wide range of pharmacologic and oncologic concerns on both experimental and clinical levels, Cancer Chemotherapy and Pharmacology is an eminent journal in the field. The primary focus in this rapid publication medium is on new anticancer agents, their experimental screening, preclinical toxicology and pharmacology, single and combined drug administration modalities, and clinical phase I, II and III trials. It is essential reading for pharmacologists and oncologists giving results recorded in the following areas: clinical toxicology, pharmacokinetics, pharmacodynamics, drug interactions, and indications for chemotherapy in cancer treatment strategy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


