Prognostic implication of heart failure stage and left ventricular ejection fraction for patients with in-hospital cardiac arrest: a 16-year retrospective cohort study.
{"title":"Prognostic implication of heart failure stage and left ventricular ejection fraction for patients with in-hospital cardiac arrest: a 16-year retrospective cohort study.","authors":"Chih-Hung Wang, Li-Ting Ho, Meng-Che Wu, Cheng-Yi Wu, Joyce Tay, Pei-I Su, Min-Shan Tsai, Yen-Wen Wu, Wei-Tien Chang, Chien-Hua Huang, Wen-Jone Chen","doi":"10.1007/s00392-024-02403-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The 2022 AHA/ACC/HFSA guidelines for the management of heart failure (HF) makes therapeutic recommendations based on HF status. We investigated whether the prognosis of in-hospital cardiac arrest (IHCA) could be stratified by HF stage and left ventricular ejection fraction (LVEF).</p><p><strong>Methods: </strong>This single-center retrospective study analyzed the data of patients who experienced IHCA between 2005 and 2020. Based on admission diagnosis, past medical records, and pre-arrest echocardiography, patients were classified into general IHCA, at-risk for HF, pre-HF, HF with preserved ejection fraction (HFpEF), and HF with mildly reduced ejection fraction or HF with reduced ejection fraction (HFmrEF-or-HFrEF) groups.</p><p><strong>Results: </strong>This study included 2,466 patients, including 485 (19.7%), 546 (22.1%), 863 (35.0%), 342 (13.9%), and 230 (9.3%) patients with general IHCA, at-risk for HF, pre-HF, HFpEF, and HFmrEF-or-HFrEF, respectively. A total of 405 (16.4%) patients survived to hospital discharge, with 228 (9.2%) patients achieving favorable neurological recovery. Multivariable logistic regression analysis indicated that pre-HF and HFpEF were associated with better neurological (pre-HF, OR: 2.11, 95% confidence interval [CI]: 1.23-3.61, p = 0.006; HFpEF, OR: 1.90, 95% CI: 1.00-3.61, p = 0.05) and survival outcomes (pre-HF, OR: 2.00, 95% CI: 1.34-2.97, p < 0.001; HFpEF, OR: 1.91, 95% CI: 1.20-3.05, p = 0.007), compared with general IHCA.</p><p><strong>Conclusion: </strong>HF stage and LVEF could stratify patients with IHCA into different prognoses. Pre-HF and HFpEF were significantly associated with favorable neurological and survival outcomes after IHCA. Further studies are warranted to investigate whether HF status-directed management could improve IHCA outcomes.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"557-569"},"PeriodicalIF":3.8000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058836/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02403-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The 2022 AHA/ACC/HFSA guidelines for the management of heart failure (HF) makes therapeutic recommendations based on HF status. We investigated whether the prognosis of in-hospital cardiac arrest (IHCA) could be stratified by HF stage and left ventricular ejection fraction (LVEF).
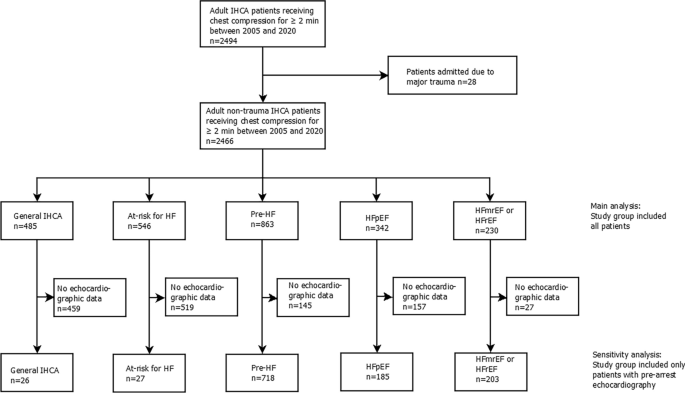
Methods: This single-center retrospective study analyzed the data of patients who experienced IHCA between 2005 and 2020. Based on admission diagnosis, past medical records, and pre-arrest echocardiography, patients were classified into general IHCA, at-risk for HF, pre-HF, HF with preserved ejection fraction (HFpEF), and HF with mildly reduced ejection fraction or HF with reduced ejection fraction (HFmrEF-or-HFrEF) groups.
Results: This study included 2,466 patients, including 485 (19.7%), 546 (22.1%), 863 (35.0%), 342 (13.9%), and 230 (9.3%) patients with general IHCA, at-risk for HF, pre-HF, HFpEF, and HFmrEF-or-HFrEF, respectively. A total of 405 (16.4%) patients survived to hospital discharge, with 228 (9.2%) patients achieving favorable neurological recovery. Multivariable logistic regression analysis indicated that pre-HF and HFpEF were associated with better neurological (pre-HF, OR: 2.11, 95% confidence interval [CI]: 1.23-3.61, p = 0.006; HFpEF, OR: 1.90, 95% CI: 1.00-3.61, p = 0.05) and survival outcomes (pre-HF, OR: 2.00, 95% CI: 1.34-2.97, p < 0.001; HFpEF, OR: 1.91, 95% CI: 1.20-3.05, p = 0.007), compared with general IHCA.
Conclusion: HF stage and LVEF could stratify patients with IHCA into different prognoses. Pre-HF and HFpEF were significantly associated with favorable neurological and survival outcomes after IHCA. Further studies are warranted to investigate whether HF status-directed management could improve IHCA outcomes.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


