Evaluation of nocturnal apnea and airflow limitation as indicators for cognitive dysfunction in patients with chronic obstructive pulmonary disease/obstructive sleep apnea hypopnea syndrome overlap syndrome.
{"title":"Evaluation of nocturnal apnea and airflow limitation as indicators for cognitive dysfunction in patients with chronic obstructive pulmonary disease/obstructive sleep apnea hypopnea syndrome overlap syndrome.","authors":"Zheng Zhu, Yaohua Wu, Ling Qu, Ying Zou, Guozhong Nie, Shuguang Xu, Qixing Zhou, Yunfeng Zhang, Rui Chen","doi":"10.1177/14799731241236492","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this study is to investigate how much intermittent hypoxemia and airflow limitation contribute to cognitive impairment in overlap syndrome (OS), which is the coexistence of two common diseases, obstructive sleep apnea hypopnea syndrome (OSAHS) and chronic obstructive pulmonary disease (COPD).</p><p><strong>Methods: </strong>We conducted a cross-sectional study of patients with OSAHS, COPD or OS, compared with normal controls, to determine the association between sleep apnea/pulmonary function-related indicators and cognitive dysfunction in individuals with OSAHS, COPD or OS.</p><p><strong>Results: </strong>A total of 157 participants were recruited. Both OSAHS and OS presented lower adjusted Montreal cognitive assessment (MoCA) scores compared with COPD group. In addition, the MoCA score was significantly lower in COPD group compared with control group. The incidence of cognitive impairment was 57.4% in OSAHS group, and 78% in OS group, which were significantly higher than COPD group (29%) and control group (8.8%). Furthermore, a broader range of cognitive domains were affected in OS group compared with OSAHS group. Elevated levels of oxygen desaturation index (ODI) and/or apnea hypopnea index (AHI) were positively correlated with increased Epworth sleeping scale (ESS) in OSAHS and OS. Forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1) and peak expiratory flow (PEF) were positively correlated with cognitive scores in OSAHS but not in OS. Serum level of hypoxia-inducible factor-1α (HIF-1α) was significantly higher in OS. Logistic regression identified ODI as an independent risk factor for cognitive impairment in OS, while severity of snoring and PEF were independent risk factors in OSAHS.</p><p><strong>Discussion: </strong>This study revealed significant cognitive impairment in OS, OSAHS and COPD. Sleep-related indicators are warranted in OS patients for detection, differentiation and grading of cognitive impairment, whereas pulmonary functions are warranted in OSAHS patients for detection and early intervention of cognitive impairment.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"21 ","pages":"14799731241236492"},"PeriodicalIF":2.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10901067/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731241236492","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The aim of this study is to investigate how much intermittent hypoxemia and airflow limitation contribute to cognitive impairment in overlap syndrome (OS), which is the coexistence of two common diseases, obstructive sleep apnea hypopnea syndrome (OSAHS) and chronic obstructive pulmonary disease (COPD).
Methods: We conducted a cross-sectional study of patients with OSAHS, COPD or OS, compared with normal controls, to determine the association between sleep apnea/pulmonary function-related indicators and cognitive dysfunction in individuals with OSAHS, COPD or OS.
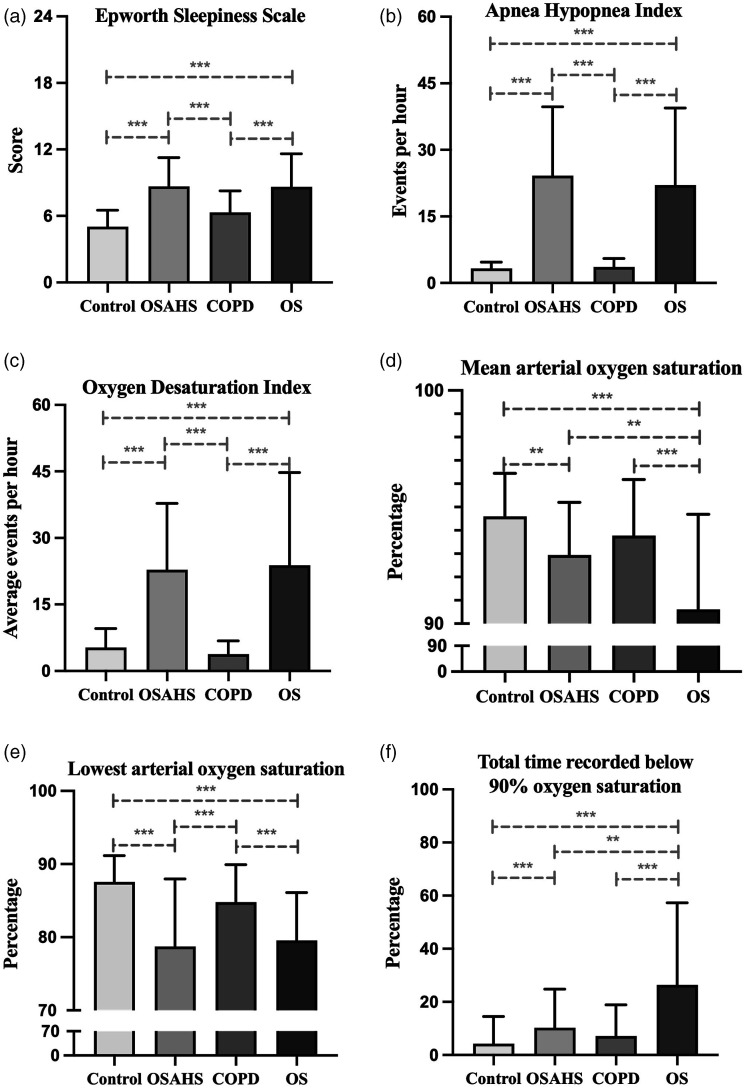
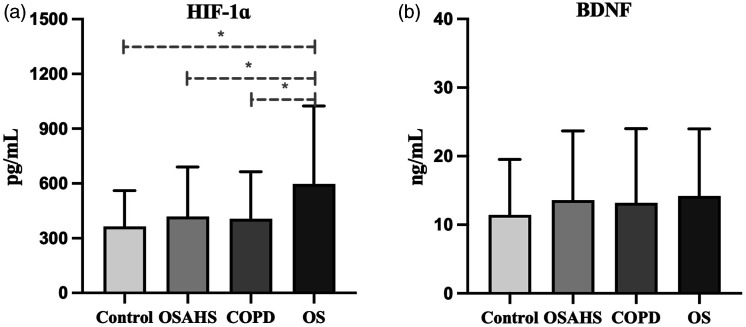
Results: A total of 157 participants were recruited. Both OSAHS and OS presented lower adjusted Montreal cognitive assessment (MoCA) scores compared with COPD group. In addition, the MoCA score was significantly lower in COPD group compared with control group. The incidence of cognitive impairment was 57.4% in OSAHS group, and 78% in OS group, which were significantly higher than COPD group (29%) and control group (8.8%). Furthermore, a broader range of cognitive domains were affected in OS group compared with OSAHS group. Elevated levels of oxygen desaturation index (ODI) and/or apnea hypopnea index (AHI) were positively correlated with increased Epworth sleeping scale (ESS) in OSAHS and OS. Forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1) and peak expiratory flow (PEF) were positively correlated with cognitive scores in OSAHS but not in OS. Serum level of hypoxia-inducible factor-1α (HIF-1α) was significantly higher in OS. Logistic regression identified ODI as an independent risk factor for cognitive impairment in OS, while severity of snoring and PEF were independent risk factors in OSAHS.
Discussion: This study revealed significant cognitive impairment in OS, OSAHS and COPD. Sleep-related indicators are warranted in OS patients for detection, differentiation and grading of cognitive impairment, whereas pulmonary functions are warranted in OSAHS patients for detection and early intervention of cognitive impairment.
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


