Severe Hypercalcemia Caused by Calcium-Alkali Syndrome after 15 Years of Postoperative Hypoparathyroidism in a Patient with Undiagnosed Hyperaldosteronism.
Natália Diel Boufleuer, Dimitris V Rados, Tatiana Zambonato, Clara K Maraschin, Beatriz D Schaan
{"title":"Severe Hypercalcemia Caused by Calcium-Alkali Syndrome after 15 Years of Postoperative Hypoparathyroidism in a Patient with Undiagnosed Hyperaldosteronism.","authors":"Natália Diel Boufleuer, Dimitris V Rados, Tatiana Zambonato, Clara K Maraschin, Beatriz D Schaan","doi":"10.1155/2024/3067354","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The triad of hypercalcemia, metabolic alkalosis, and acute kidney injury associated with ingesting high doses of calcium and absorbable bases characterizes the calcium-alkali syndrome. <i>Clinical Case</i>. We report the case of a patient with postthyroidectomy hypoparathyroidism 15 years ago due to differentiated thyroid cancer who presented with severe hypercalcemia. He had adequate control of calcemia for many years on treatment with calcitriol and calcium carbonate and hypertension treated with amlodipine, losartan, and hydrochlorothiazide. After a period of loss to follow-up, he suddenly presents with severe hypercalcemia, metabolic alkalosis, and loss of renal function. Upon hydration and withdrawal of calcitriol and calcium replacements, hypercalcemia resolved. The etiological investigation identified no granulomatous or neoplastic diseases, but an aldosterone-producing adrenal incidentaloma was found. The cause of hypercalcemia in this patient was calcium-alkali syndrome due to calcium carbonate replacement potentiated by hydrochlorothiazide and primary aldosteronism. Six months after the hospitalization and suspension of calcium and vitamin D, the patient returned to hypocalcemia, reinforcing the diagnosis.</p><p><strong>Conclusion: </strong>Although seldom described, the calcium-alkali syndrome is an expected complication for individuals with postoperative hypoparathyroidism, as they require lifelong calcium and vitamin D supplementation. This case also shows the importance of hydrochlorothiazide use and primary aldosteronism as possible triggers of life-threatening hypercalcemia.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"3067354"},"PeriodicalIF":0.9000,"publicationDate":"2024-02-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10890900/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/3067354","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
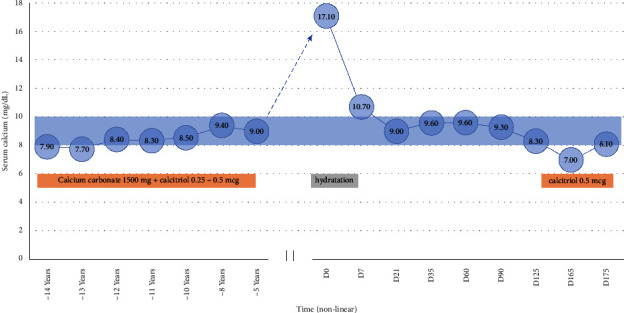
Introduction: The triad of hypercalcemia, metabolic alkalosis, and acute kidney injury associated with ingesting high doses of calcium and absorbable bases characterizes the calcium-alkali syndrome. Clinical Case. We report the case of a patient with postthyroidectomy hypoparathyroidism 15 years ago due to differentiated thyroid cancer who presented with severe hypercalcemia. He had adequate control of calcemia for many years on treatment with calcitriol and calcium carbonate and hypertension treated with amlodipine, losartan, and hydrochlorothiazide. After a period of loss to follow-up, he suddenly presents with severe hypercalcemia, metabolic alkalosis, and loss of renal function. Upon hydration and withdrawal of calcitriol and calcium replacements, hypercalcemia resolved. The etiological investigation identified no granulomatous or neoplastic diseases, but an aldosterone-producing adrenal incidentaloma was found. The cause of hypercalcemia in this patient was calcium-alkali syndrome due to calcium carbonate replacement potentiated by hydrochlorothiazide and primary aldosteronism. Six months after the hospitalization and suspension of calcium and vitamin D, the patient returned to hypocalcemia, reinforcing the diagnosis.
Conclusion: Although seldom described, the calcium-alkali syndrome is an expected complication for individuals with postoperative hypoparathyroidism, as they require lifelong calcium and vitamin D supplementation. This case also shows the importance of hydrochlorothiazide use and primary aldosteronism as possible triggers of life-threatening hypercalcemia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


