Elizabeth M. Camacho, Katherine J. Gold, Margaret Murphy, Claire Storey, Alexander E. P. Heazell
{"title":"Measuring EQ-5D-5L utility values in parents who have experienced perinatal death","authors":"Elizabeth M. Camacho, Katherine J. Gold, Margaret Murphy, Claire Storey, Alexander E. P. Heazell","doi":"10.1007/s10198-024-01677-z","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Policymakers use clinical and cost-effectiveness evidence to support decisions about health service commissioning. In England, the National Institute for Health and Care Excellence (NICE) recommend that in cost-effectiveness analyses “effectiveness” is measured as quality-adjusted life years (QALYs), derived from health utility values. The impact of perinatal death (stillbirth/neonatal death) on parents’ health utility is currently unknown. This knowledge would improve the robustness of cost-effectiveness evidence for policymakers.</p><h3 data-test=\"abstract-sub-heading\">Objective</h3><p>This study aimed to estimate the impact of perinatal death on parents’ health utility.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>An online survey conducted with mothers and fathers in England who experienced a perinatal death. Participants reported how long ago their baby died and whether they/their partner subsequently became pregnant again. They were asked to rate their health on the EQ-5D-5L instrument (generic health measure). EQ-5D-5L responses were used to calculate health utility values. These were compared with age-matched values for the general population to estimate a utility shortfall (i.e. health loss) associated with perinatal death.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>There were 256 survey respondents with a median age of 40 years (IQR 26–40). Median time since death was 27 months (IQR 8–71). The mean utility value of the sample was 0.774 (95% CI 0.752–0.796). Utility values in the sample were 13% lower than general population values (<i>p</i> < 0.05). Over 10 years, this equated to a loss of 1.1 QALYs. This reduction in health utility was driven by anxiety and depression.</p><h3 data-test=\"abstract-sub-heading\">Conclusions</h3><p>Perinatal death has important and long-lasting health impacts on parents. Mental health support following perinatal bereavement is especially important.</p>","PeriodicalId":22450,"journal":{"name":"The European Journal of Health Economics","volume":"175 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The European Journal of Health Economics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10198-024-01677-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Policymakers use clinical and cost-effectiveness evidence to support decisions about health service commissioning. In England, the National Institute for Health and Care Excellence (NICE) recommend that in cost-effectiveness analyses “effectiveness” is measured as quality-adjusted life years (QALYs), derived from health utility values. The impact of perinatal death (stillbirth/neonatal death) on parents’ health utility is currently unknown. This knowledge would improve the robustness of cost-effectiveness evidence for policymakers.
Objective
This study aimed to estimate the impact of perinatal death on parents’ health utility.
Methods
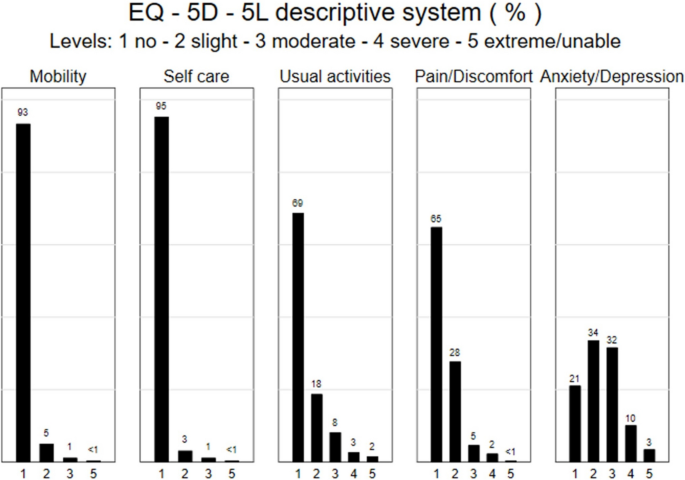
An online survey conducted with mothers and fathers in England who experienced a perinatal death. Participants reported how long ago their baby died and whether they/their partner subsequently became pregnant again. They were asked to rate their health on the EQ-5D-5L instrument (generic health measure). EQ-5D-5L responses were used to calculate health utility values. These were compared with age-matched values for the general population to estimate a utility shortfall (i.e. health loss) associated with perinatal death.
Results
There were 256 survey respondents with a median age of 40 years (IQR 26–40). Median time since death was 27 months (IQR 8–71). The mean utility value of the sample was 0.774 (95% CI 0.752–0.796). Utility values in the sample were 13% lower than general population values (p < 0.05). Over 10 years, this equated to a loss of 1.1 QALYs. This reduction in health utility was driven by anxiety and depression.
Conclusions
Perinatal death has important and long-lasting health impacts on parents. Mental health support following perinatal bereavement is especially important.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


