Urszula Żebrowska, Walentyna Balwierz, Jarosław Wechowski, Aleksandra Wieczorek
{"title":"Survival Benefit of Myeloablative Therapy with Autologous Stem Cell Transplantation in High-Risk Neuroblastoma: A Systematic Literature Review.","authors":"Urszula Żebrowska, Walentyna Balwierz, Jarosław Wechowski, Aleksandra Wieczorek","doi":"10.1007/s11523-024-01033-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multimodal treatment of newly diagnosed high-risk neuroblastoma (HRNB) includes induction chemotherapy, consolidation with myeloablative therapy (MAT) and autologous stem cell transplantation (ASCT), followed by anti-disialoganglioside 2 (GD2) immunotherapy, as recommended by the Children's Oncology Group (COG) and the Society of Paediatric Oncology European Neuroblastoma (SIOPEN). Some centres proposed an alternative approach with induction chemotherapy followed by anti-GD2 immunotherapy, without MAT+ASCT.</p><p><strong>Objective: </strong>The aim of this systematic literature review was to compare survival outcomes in patients with HRNB treated with or without MAT+ASCT and with or without subsequent anti-GD2 immunotherapy.</p><p><strong>Patients and methods: </strong>The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. MEDLINE via PubMed and EMBASE databases were systematically searched for randomised controlled trials (RCT) and observational comparative studies in patients with HRNB using search terms for 'neuroblastoma' and ('myeloablative therapy' OR 'stem cell transplantation'). Reporting of at least one survival outcome [event-free survival (EFS), progression-free survival, relapse-free survival and/or overall survival (OS)] was required for inclusion. Outcomes from RCTs were synthesized in meta-analysis, while meta-analysis of non-RCTs was not planned owing to expected heterogeneity.</p><p><strong>Results: </strong>Literature searches produced 2587 results with 41 publications reporting 34 comparative studies included in the review. Of these, 7 publications reported 4 RCTs, and 34 publications reported 30 non-RCT studies. Studies differed with respect to included populations, induction regimen, response to induction, additional treatments and transplantation procedures. Subsequent treatments of relapse were rarely reported and could not be compared. In the meta-analysis, EFS was in favour of MAT+ASCT over conventional chemotherapy or no further treatment [hazard ratio (HR) = 0.78, 95% confidence interval (CI) 0.67-0.91, p = 0.001] with a trend favouring MAT+ASCT for OS (HR = 0.86, 95% CI 0.73-1.00, p = 0.05). Tandem MAT+ASCT was found to improve EFS compared with the single procedure, with improvement in both EFS and OS in patients treated with anti-GD2 therapy. Non-RCT comparative studies were broadly consistent with evidence from the RCTs; however, not all reported survival benefits of MAT+ASCT (single or tandem). Limited comparative evidence on treatment without MAT+ASCT in patients treated with anti-GD2 immunotherapy suggests an increased risk of relapse. In relapsed patients, MAT+ASCT appears to improve OS, but evidence remains scarce.</p><p><strong>Conclusions: </strong>Survival benefits in patients treated with MAT+ASCT confirm that the procedure should remain an integral part of multimodal therapy. In patients treated with anti-GD2 immunotherapy, limited evidence suggests that omitting MAT+ASCT is associated with an increased risk of relapse, and therefore, a change in clinical practice can currently not be recommended. Evidence suggests the use of tandem MAT+ASCT compared with the single procedure, with greater benefits observed in patients treated with anti-GD2 immunotherapy. Limited evidence also suggests improved survival following MAT+ASCT in relapsed patients, which needs to be viewed in light of emerging chemoimmunotherapy in this setting.</p>","PeriodicalId":22195,"journal":{"name":"Targeted Oncology","volume":" ","pages":"143-159"},"PeriodicalIF":4.4000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10963547/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Targeted Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11523-024-01033-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Multimodal treatment of newly diagnosed high-risk neuroblastoma (HRNB) includes induction chemotherapy, consolidation with myeloablative therapy (MAT) and autologous stem cell transplantation (ASCT), followed by anti-disialoganglioside 2 (GD2) immunotherapy, as recommended by the Children's Oncology Group (COG) and the Society of Paediatric Oncology European Neuroblastoma (SIOPEN). Some centres proposed an alternative approach with induction chemotherapy followed by anti-GD2 immunotherapy, without MAT+ASCT.
Objective: The aim of this systematic literature review was to compare survival outcomes in patients with HRNB treated with or without MAT+ASCT and with or without subsequent anti-GD2 immunotherapy.
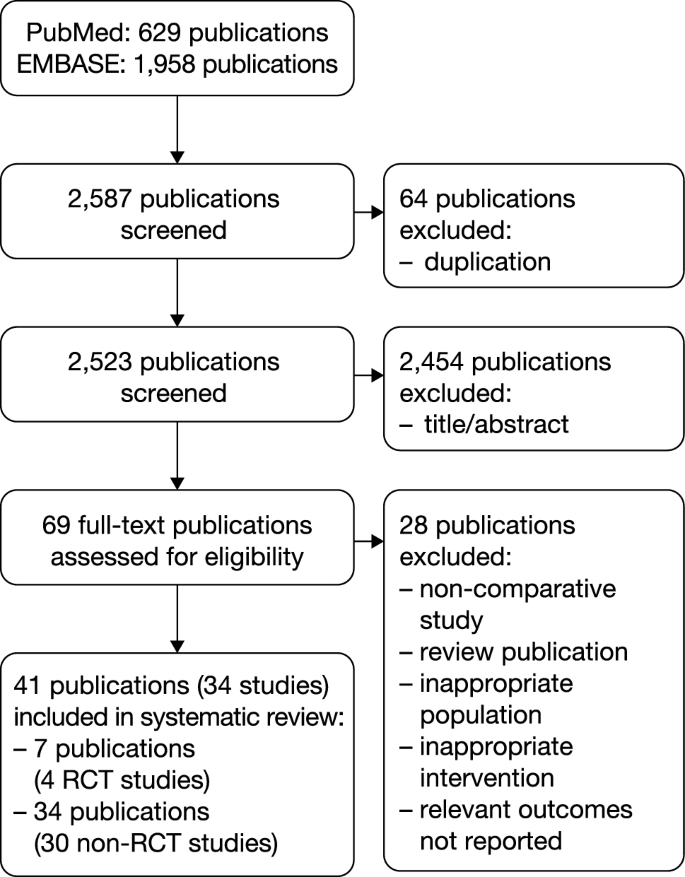
Patients and methods: The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. MEDLINE via PubMed and EMBASE databases were systematically searched for randomised controlled trials (RCT) and observational comparative studies in patients with HRNB using search terms for 'neuroblastoma' and ('myeloablative therapy' OR 'stem cell transplantation'). Reporting of at least one survival outcome [event-free survival (EFS), progression-free survival, relapse-free survival and/or overall survival (OS)] was required for inclusion. Outcomes from RCTs were synthesized in meta-analysis, while meta-analysis of non-RCTs was not planned owing to expected heterogeneity.
Results: Literature searches produced 2587 results with 41 publications reporting 34 comparative studies included in the review. Of these, 7 publications reported 4 RCTs, and 34 publications reported 30 non-RCT studies. Studies differed with respect to included populations, induction regimen, response to induction, additional treatments and transplantation procedures. Subsequent treatments of relapse were rarely reported and could not be compared. In the meta-analysis, EFS was in favour of MAT+ASCT over conventional chemotherapy or no further treatment [hazard ratio (HR) = 0.78, 95% confidence interval (CI) 0.67-0.91, p = 0.001] with a trend favouring MAT+ASCT for OS (HR = 0.86, 95% CI 0.73-1.00, p = 0.05). Tandem MAT+ASCT was found to improve EFS compared with the single procedure, with improvement in both EFS and OS in patients treated with anti-GD2 therapy. Non-RCT comparative studies were broadly consistent with evidence from the RCTs; however, not all reported survival benefits of MAT+ASCT (single or tandem). Limited comparative evidence on treatment without MAT+ASCT in patients treated with anti-GD2 immunotherapy suggests an increased risk of relapse. In relapsed patients, MAT+ASCT appears to improve OS, but evidence remains scarce.
Conclusions: Survival benefits in patients treated with MAT+ASCT confirm that the procedure should remain an integral part of multimodal therapy. In patients treated with anti-GD2 immunotherapy, limited evidence suggests that omitting MAT+ASCT is associated with an increased risk of relapse, and therefore, a change in clinical practice can currently not be recommended. Evidence suggests the use of tandem MAT+ASCT compared with the single procedure, with greater benefits observed in patients treated with anti-GD2 immunotherapy. Limited evidence also suggests improved survival following MAT+ASCT in relapsed patients, which needs to be viewed in light of emerging chemoimmunotherapy in this setting.
期刊介绍:
Targeted Oncology addresses physicians and scientists committed to oncology and cancer research by providing a programme of articles on molecularly targeted pharmacotherapy in oncology. The journal includes:
Original Research Articles on all aspects of molecularly targeted agents for the treatment of cancer, including immune checkpoint inhibitors and related approaches.
Comprehensive narrative Review Articles and shorter Leading Articles discussing relevant clinically established as well as emerging agents and pathways.
Current Opinion articles that place interesting areas in perspective.
Therapy in Practice articles that provide a guide to the optimum management of a condition and highlight practical, clinically relevant considerations and recommendations.
Systematic Reviews that use explicit, systematic methods as outlined by the PRISMA statement.
Adis Drug Reviews of the properties and place in therapy of both newer and established targeted drugs in oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


