Isatuximab in combination with carfilzomib and dexamethasone in 1q21+ patients with relapsed/refractory multiple myeloma: Long-term outcomes in the Phase 3 IKEMA study
Thierry Facon, Philippe Moreau, Ivan Špicka, Kenshi Suzuki, Kwee Yong, Joseph Mikhael, Taro Fukao, Kamlesh Bisht, Nicole M. Armstrong, Sandrine Macé, Marie-Laure Risse, Thomas Martin
{"title":"Isatuximab in combination with carfilzomib and dexamethasone in 1q21+ patients with relapsed/refractory multiple myeloma: Long-term outcomes in the Phase 3 IKEMA study","authors":"Thierry Facon, Philippe Moreau, Ivan Špicka, Kenshi Suzuki, Kwee Yong, Joseph Mikhael, Taro Fukao, Kamlesh Bisht, Nicole M. Armstrong, Sandrine Macé, Marie-Laure Risse, Thomas Martin","doi":"10.1002/hon.3258","DOIUrl":null,"url":null,"abstract":"<p>Gain/amplification of 1q21 (≥3 copies), a chromosomal abnormality frequently observed in multiple myeloma, can negatively affect prognosis, due to its involvement in resistance to anti-myeloma therapy and disease progression. In this updated subgroup analysis of the randomized, Phase 3 IKEMA study (NCT03275285) in relapsed/refractory multiple myeloma (RRMM), we evaluated progression-free survival (PFS) and depth of response with the anti-CD38 antibody isatuximab plus carfilzomib-dexamethasone (Isa-Kd) versus Kd, in 1q21+ patients and related subgroups, at long-term follow-up (44.2 months). Our analysis included patients with 1q21+ (≥3 copies, with/without high-risk chromosomal abnormality [HRCA]), isolated 1q21+ (≥3 copies, without HRCA), gain(1q21) (3 copies, with/without HRCA), and amp(1q21) (≥4 copies, with/without HRCA). PFS benefit was achieved with Isa-Kd versus Kd in patients with 1q21+ (HR 0.58, 95% CI: 0.37–0.92), with isolated 1q21+ (HR 0.49, 95% CI: 0.27–0.92), with gain(1q21), or amp(1q21), consistent with the overall population and prior interim 1q21+ subgroup analyses. Median PFS with Isa-Kd versus Kd was 25.8 versus 16.2 months in 1q21+ patients and 38.2 versus 16.2 months in patients with isolated 1q21+. Clinically meaningful, higher rates of very good partial response or better, complete response or better (≥CR), minimal residual disease (MRD) negativity, and MRD negativity and ≥CR were reached with Isa-Kd versus Kd in patients with 1q21+, isolated 1q21+, gain(1q21), or amp(1q21). In Isa-Kd and Kd, the MRD negativity and ≥CR rate was 29.3% versus 15.4% in 1q21+ patients, 36.2% versus 12.9% in patients with isolated 1q21+, 27.9% versus 13.5% in patients with gain(1q21), and 31.3% versus 20.0% in patients with amp(1q21), respectively. In conclusion, addition of Isa to Kd in triplet combination therapy has shown PFS benefit and deeper responses, compared with Kd, in 1q21+ patients at higher risk of progression, including patients with isolated 1q21+, gain(1q21), and amp(1q21), thus supporting Isa-Kd an effective treatment option for patients with RRMM.</p>","PeriodicalId":12882,"journal":{"name":"Hematological Oncology","volume":"42 2","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2024-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3258","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematological Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hon.3258","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
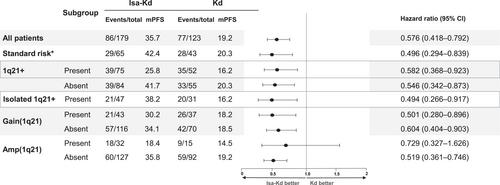
Gain/amplification of 1q21 (≥3 copies), a chromosomal abnormality frequently observed in multiple myeloma, can negatively affect prognosis, due to its involvement in resistance to anti-myeloma therapy and disease progression. In this updated subgroup analysis of the randomized, Phase 3 IKEMA study (NCT03275285) in relapsed/refractory multiple myeloma (RRMM), we evaluated progression-free survival (PFS) and depth of response with the anti-CD38 antibody isatuximab plus carfilzomib-dexamethasone (Isa-Kd) versus Kd, in 1q21+ patients and related subgroups, at long-term follow-up (44.2 months). Our analysis included patients with 1q21+ (≥3 copies, with/without high-risk chromosomal abnormality [HRCA]), isolated 1q21+ (≥3 copies, without HRCA), gain(1q21) (3 copies, with/without HRCA), and amp(1q21) (≥4 copies, with/without HRCA). PFS benefit was achieved with Isa-Kd versus Kd in patients with 1q21+ (HR 0.58, 95% CI: 0.37–0.92), with isolated 1q21+ (HR 0.49, 95% CI: 0.27–0.92), with gain(1q21), or amp(1q21), consistent with the overall population and prior interim 1q21+ subgroup analyses. Median PFS with Isa-Kd versus Kd was 25.8 versus 16.2 months in 1q21+ patients and 38.2 versus 16.2 months in patients with isolated 1q21+. Clinically meaningful, higher rates of very good partial response or better, complete response or better (≥CR), minimal residual disease (MRD) negativity, and MRD negativity and ≥CR were reached with Isa-Kd versus Kd in patients with 1q21+, isolated 1q21+, gain(1q21), or amp(1q21). In Isa-Kd and Kd, the MRD negativity and ≥CR rate was 29.3% versus 15.4% in 1q21+ patients, 36.2% versus 12.9% in patients with isolated 1q21+, 27.9% versus 13.5% in patients with gain(1q21), and 31.3% versus 20.0% in patients with amp(1q21), respectively. In conclusion, addition of Isa to Kd in triplet combination therapy has shown PFS benefit and deeper responses, compared with Kd, in 1q21+ patients at higher risk of progression, including patients with isolated 1q21+, gain(1q21), and amp(1q21), thus supporting Isa-Kd an effective treatment option for patients with RRMM.
期刊介绍:
Hematological Oncology considers for publication articles dealing with experimental and clinical aspects of neoplastic diseases of the hemopoietic and lymphoid systems and relevant related matters. Translational studies applying basic science to clinical issues are particularly welcomed. Manuscripts dealing with the following areas are encouraged:
-Clinical practice and management of hematological neoplasia, including: acute and chronic leukemias, malignant lymphomas, myeloproliferative disorders
-Diagnostic investigations, including imaging and laboratory assays
-Epidemiology, pathology and pathobiology of hematological neoplasia of hematological diseases
-Therapeutic issues including Phase 1, 2 or 3 trials as well as allogeneic and autologous stem cell transplantation studies
-Aspects of the cell biology, molecular biology, molecular genetics and cytogenetics of normal or diseased hematopoeisis and lymphopoiesis, including stem cells and cytokines and other regulatory systems.
Concise, topical review material is welcomed, especially if it makes new concepts and ideas accessible to a wider community. Proposals for review material may be discussed with the Editor-in-Chief. Collections of case material and case reports will be considered only if they have broader scientific or clinical relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


