{"title":"Boerhaave's Syndrome Presenting in the Setting of Third-Degree Heart Block.","authors":"Jay A Redan, Taylor Croteau, Colleen Gaughan","doi":"10.4293/CRSLS.2023.00052","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Boerhaave's syndrome, or the spontaneous transmural perforation of the esophagus, is typically thought to be due to an increase in esophageal pressure such as that which occurs during vomiting or retching. Another common etiology of esophageal perforation is esophageal instrumentation, such as during esophagogastroduodenoscopy or transesophageal echocardiography. This life-threatening condition requires prompt diagnosis and treatment to prevent patient demise. While a history of vomiting can aid in diagnosis, this history can be difficult to elicit in an unconscious patient or may be altogether absent. Additionally, Boerhaave's syndrome can present similarly to more common upper gastrointestinal or cardiac conditions. Since mortality increases with delays in diagnosis and treatment, it is imperative that clinicians maintain a high level of suspicion for Boerhaave's syndrome and initiate treatment urgently.</p><p><strong>Case description: </strong>This report presents a 76-year-old man who presented to the emergency department after a history of several syncopal episodes and was found to be in complete heart block. Two days later, he acutely developed abdominal distention and coffee ground emesis. As the medical team was able to gather more history from the patient and his family, it was revealed that he had associated vomiting with his episodes of syncope. CT scan of the abdomen and pelvis demonstrated pneumomediastinum concerning for esophageal perforation. His clinical status subsequently deteriorated. He was intubated and a temporary transvenous pacer was placed before being transferred to our facility for emergent surgery.</p><p><strong>Discussion: </strong>Complete heart block in the setting of Boerhaave's syndrome is exceptionally rare, with only 2 cases reported in the literature. The decision to place a pacemaker in the setting of esophageal perforation/sepsis is complicated and depends on the patient's bacteremia status related to noncardiac comorbidities. Clearly this case represents the need for excellent multidisciplinary decision-making processes with excellent communication between hospital staff and all caretakers. Expeditious diagnosis and treatment of esophageal perforation is essential to prevent leaking of gastric contents into the mediastinum and worsening of cardiac complications and sepsis. Additionally, critical timing of various surgical procedures, especially the need for a permanent pacemaker implant with bacteremia is a complicated process not well described in the surgical literature.</p>","PeriodicalId":72723,"journal":{"name":"CRSLS : MIS case reports from SLS","volume":"11 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10880586/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CRSLS : MIS case reports from SLS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4293/CRSLS.2023.00052","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Boerhaave's syndrome, or the spontaneous transmural perforation of the esophagus, is typically thought to be due to an increase in esophageal pressure such as that which occurs during vomiting or retching. Another common etiology of esophageal perforation is esophageal instrumentation, such as during esophagogastroduodenoscopy or transesophageal echocardiography. This life-threatening condition requires prompt diagnosis and treatment to prevent patient demise. While a history of vomiting can aid in diagnosis, this history can be difficult to elicit in an unconscious patient or may be altogether absent. Additionally, Boerhaave's syndrome can present similarly to more common upper gastrointestinal or cardiac conditions. Since mortality increases with delays in diagnosis and treatment, it is imperative that clinicians maintain a high level of suspicion for Boerhaave's syndrome and initiate treatment urgently.
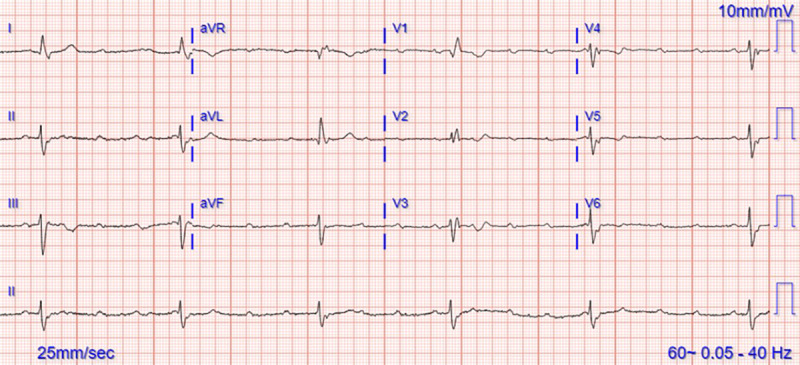
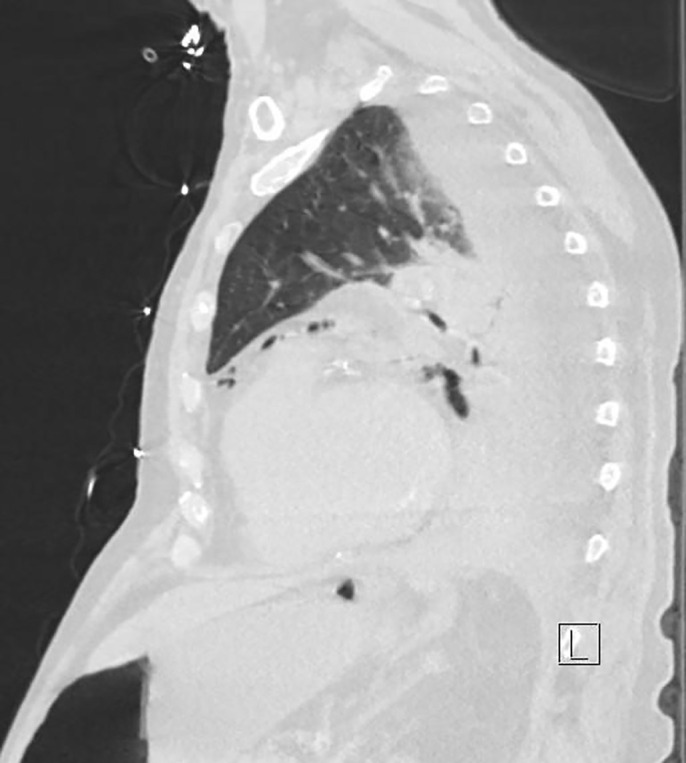
Case description: This report presents a 76-year-old man who presented to the emergency department after a history of several syncopal episodes and was found to be in complete heart block. Two days later, he acutely developed abdominal distention and coffee ground emesis. As the medical team was able to gather more history from the patient and his family, it was revealed that he had associated vomiting with his episodes of syncope. CT scan of the abdomen and pelvis demonstrated pneumomediastinum concerning for esophageal perforation. His clinical status subsequently deteriorated. He was intubated and a temporary transvenous pacer was placed before being transferred to our facility for emergent surgery.
Discussion: Complete heart block in the setting of Boerhaave's syndrome is exceptionally rare, with only 2 cases reported in the literature. The decision to place a pacemaker in the setting of esophageal perforation/sepsis is complicated and depends on the patient's bacteremia status related to noncardiac comorbidities. Clearly this case represents the need for excellent multidisciplinary decision-making processes with excellent communication between hospital staff and all caretakers. Expeditious diagnosis and treatment of esophageal perforation is essential to prevent leaking of gastric contents into the mediastinum and worsening of cardiac complications and sepsis. Additionally, critical timing of various surgical procedures, especially the need for a permanent pacemaker implant with bacteremia is a complicated process not well described in the surgical literature.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


