Sarah Davis, Steve Goodacre, Daniel Horner, Abdullah Pandor, Mark Holland, Kerstin de Wit, Beverley J Hunt, Xavier Luke Griffin
{"title":"Effectiveness and cost effectiveness of pharmacological thromboprophylaxis for medical inpatients: decision analysis modelling study.","authors":"Sarah Davis, Steve Goodacre, Daniel Horner, Abdullah Pandor, Mark Holland, Kerstin de Wit, Beverley J Hunt, Xavier Luke Griffin","doi":"10.1136/bmjmed-2022-000408","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To determine the balance of costs, risks, and benefits for different thromboprophylaxis strategies for medical patients during hospital admission.</p><p><strong>Design: </strong>Decision analysis modelling study.</p><p><strong>Setting: </strong>NHS hospitals in England.</p><p><strong>Population: </strong>Eligible adult medical inpatients, excluding patients in critical care and pregnant women.</p><p><strong>Interventions: </strong>Pharmacological thromboprophylaxis (low molecular weight heparin) for all medical inpatients, thromboprophylaxis for none, and thromboprophylaxis given to higher risk inpatients according to risk assessment models (Padua, Caprini, IMPROVE, Intermountain, Kucher, Geneva, and Rothberg) previously validated in medical cohorts.</p><p><strong>Main outcome measures: </strong>Lifetime costs and quality adjusted life years (QALYs). Costs were assessed from the perspective of the NHS and Personal Social Services in England. Other outcomes assessed were incidence and treatment of venous thromboembolism, major bleeds including intracranial haemorrhage, chronic thromboembolic complications, and overall survival.</p><p><strong>Results: </strong>Offering thromboprophylaxis to all medical inpatients had a high probability (>99%) of being the most cost effective strategy (at a threshold of £20 000 (€23 440; $25 270) per QALY) in the probabilistic sensitivity analysis, when applying performance data from the Padua risk assessment model, which was typical of that observed across several risk assessment models in a medical inpatient cohort. Thromboprophylaxis for all medical inpatients was estimated to result in 0.0552 additional QALYs (95% credible interval 0.0209 to 0.1111) while generating cost savings of £28.44 (-£47 to £105) compared with thromboprophylaxis for none. No other risk assessment model was more cost effective than thromboprophylaxis for all medical inpatients when assessed in deterministic analysis. Risk based thromboprophylaxis was found to have a high (76.6%) probability of being the most cost effective strategy only when assuming a risk assessment model with very high sensitivity is available (sensitivity 99.9% and specificity 23.7% <i>v</i> base case sensitivity 49.3% and specificity 73.0%).</p><p><strong>Conclusions: </strong>Offering pharmacological thromboprophylaxis to all eligible medical inpatients appears to be the most cost effective strategy. To be cost effective, any risk assessment model would need to have a very high sensitivity resulting in widespread thromboprophylaxis in all patients except those at the very lowest risk, who could potentially avoid prophylactic anticoagulation during their hospital stay.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"3 1","pages":"e000408"},"PeriodicalIF":10.0000,"publicationDate":"2024-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10882286/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2022-000408","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To determine the balance of costs, risks, and benefits for different thromboprophylaxis strategies for medical patients during hospital admission.
Design: Decision analysis modelling study.
Setting: NHS hospitals in England.
Population: Eligible adult medical inpatients, excluding patients in critical care and pregnant women.
Interventions: Pharmacological thromboprophylaxis (low molecular weight heparin) for all medical inpatients, thromboprophylaxis for none, and thromboprophylaxis given to higher risk inpatients according to risk assessment models (Padua, Caprini, IMPROVE, Intermountain, Kucher, Geneva, and Rothberg) previously validated in medical cohorts.
Main outcome measures: Lifetime costs and quality adjusted life years (QALYs). Costs were assessed from the perspective of the NHS and Personal Social Services in England. Other outcomes assessed were incidence and treatment of venous thromboembolism, major bleeds including intracranial haemorrhage, chronic thromboembolic complications, and overall survival.
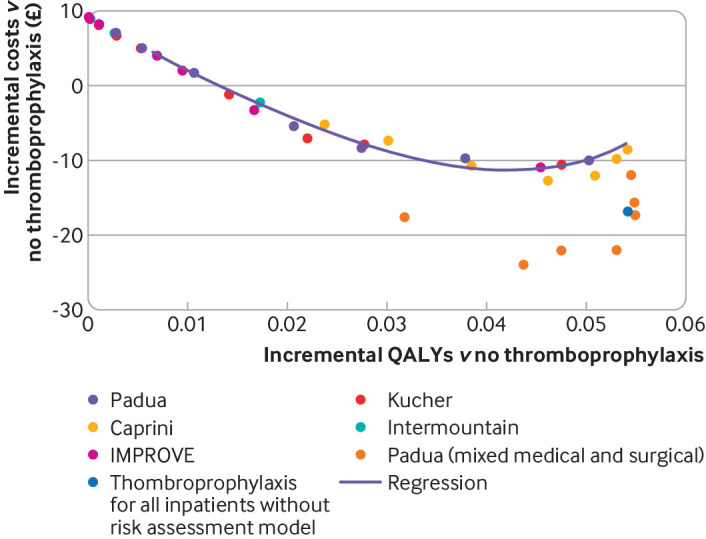
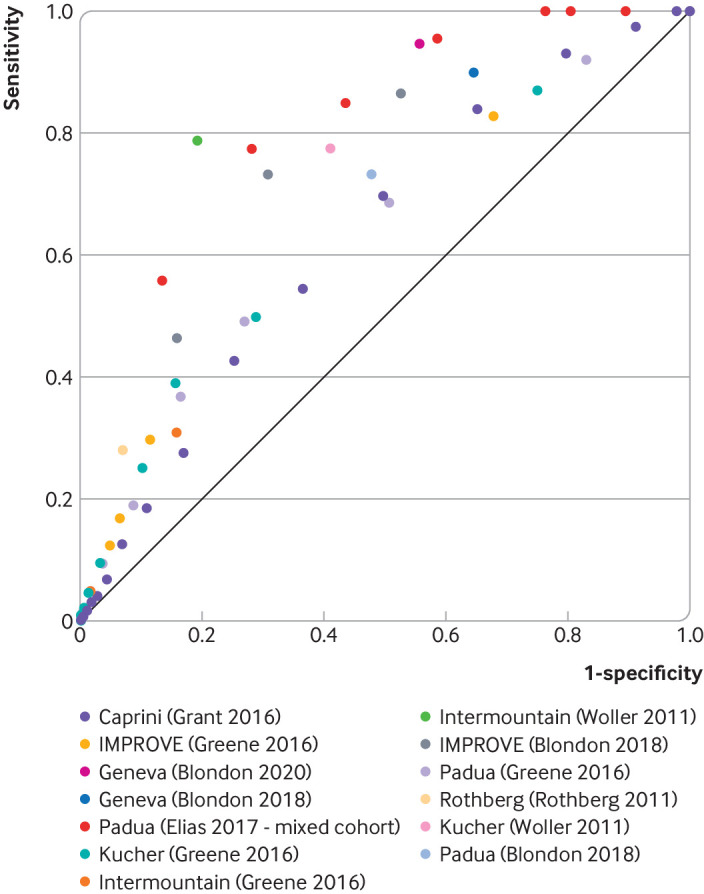
Results: Offering thromboprophylaxis to all medical inpatients had a high probability (>99%) of being the most cost effective strategy (at a threshold of £20 000 (€23 440; $25 270) per QALY) in the probabilistic sensitivity analysis, when applying performance data from the Padua risk assessment model, which was typical of that observed across several risk assessment models in a medical inpatient cohort. Thromboprophylaxis for all medical inpatients was estimated to result in 0.0552 additional QALYs (95% credible interval 0.0209 to 0.1111) while generating cost savings of £28.44 (-£47 to £105) compared with thromboprophylaxis for none. No other risk assessment model was more cost effective than thromboprophylaxis for all medical inpatients when assessed in deterministic analysis. Risk based thromboprophylaxis was found to have a high (76.6%) probability of being the most cost effective strategy only when assuming a risk assessment model with very high sensitivity is available (sensitivity 99.9% and specificity 23.7% v base case sensitivity 49.3% and specificity 73.0%).
Conclusions: Offering pharmacological thromboprophylaxis to all eligible medical inpatients appears to be the most cost effective strategy. To be cost effective, any risk assessment model would need to have a very high sensitivity resulting in widespread thromboprophylaxis in all patients except those at the very lowest risk, who could potentially avoid prophylactic anticoagulation during their hospital stay.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


