Hunter S Warwick, Timothy L Tan, Khuzaima Rangwalla, David N Shau, Jeffrey J Barry, Erik N Hansen
{"title":"Effect of Antibiotic Spacer Dosing on Treatment Success in Two-Stage Exchange for Periprosthetic Joint Infection.","authors":"Hunter S Warwick, Timothy L Tan, Khuzaima Rangwalla, David N Shau, Jeffrey J Barry, Erik N Hansen","doi":"10.5435/JAAOSGlobal-D-23-00103","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In two-stage exchange for periprosthetic joint infection (PJI), adding antibiotics to cement spacers is the standard of care; however, little is known about optimal dosage. There is emphasis on using >3.6 g of total antibiotic, including ≥2.0 g of vancomycin, per 40 g of cement, but these recommendations lack clinical evidence. We examined whether recommended antibiotic spacer doses affect treatment success.</p><p><strong>Methods: </strong>This was a retrospective review of 202 patients who underwent two-stage exchange for PJI from 2004 to 2020 with at least 1-year follow-up. Patients were separated into high (>3.6 g of total antibiotic per 40 g of cement) and low-dose spacer groups. Primary outcomes were overall and infectious failure.</p><p><strong>Results: </strong>High-dose spacers were used in 80% (162/202) of patients. High-dose spacers had a reduced risk of overall (OR, 0.37; P = 0.024) and infectious (OR, 0.35; P = 0.020) failure for infected primary arthroplasties, but not revisions. In multivariate analysis, vancomycin dose ≥2.0 g decreased the risk of infectious failure (OR, 0.31; P = 0.016), although not overall failure (OR, 0.51; P = 0.147).</p><p><strong>Conclusion: </strong>During two-stage exchange for PJI, spacers with greater than 3.6 g of total antibiotic may reduce overall and infectious failure for infected primary arthroplasties. Furthermore, using at least 2.0 g of vancomycin could independently decrease the risk of infectious failure.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"8 2","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2024-02-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10883627/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-23-00103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In two-stage exchange for periprosthetic joint infection (PJI), adding antibiotics to cement spacers is the standard of care; however, little is known about optimal dosage. There is emphasis on using >3.6 g of total antibiotic, including ≥2.0 g of vancomycin, per 40 g of cement, but these recommendations lack clinical evidence. We examined whether recommended antibiotic spacer doses affect treatment success.
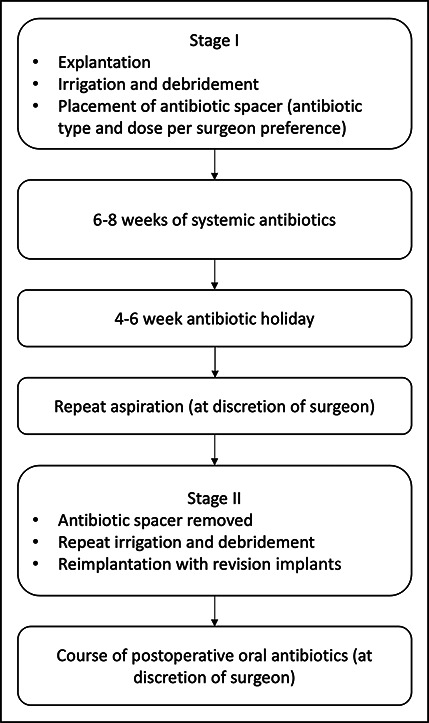
Methods: This was a retrospective review of 202 patients who underwent two-stage exchange for PJI from 2004 to 2020 with at least 1-year follow-up. Patients were separated into high (>3.6 g of total antibiotic per 40 g of cement) and low-dose spacer groups. Primary outcomes were overall and infectious failure.
Results: High-dose spacers were used in 80% (162/202) of patients. High-dose spacers had a reduced risk of overall (OR, 0.37; P = 0.024) and infectious (OR, 0.35; P = 0.020) failure for infected primary arthroplasties, but not revisions. In multivariate analysis, vancomycin dose ≥2.0 g decreased the risk of infectious failure (OR, 0.31; P = 0.016), although not overall failure (OR, 0.51; P = 0.147).
Conclusion: During two-stage exchange for PJI, spacers with greater than 3.6 g of total antibiotic may reduce overall and infectious failure for infected primary arthroplasties. Furthermore, using at least 2.0 g of vancomycin could independently decrease the risk of infectious failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


