First-line treatment of driver gene-negative metastatic lung adenocarcinoma with malignant pleural effusion: Should chemotherapy be combined with an immune checkpoint inhibitor or bevacizumab?
{"title":"First-line treatment of driver gene-negative metastatic lung adenocarcinoma with malignant pleural effusion: Should chemotherapy be combined with an immune checkpoint inhibitor or bevacizumab?","authors":"Yuanyuan Zhao, Ting Mei, Feifei Na, Xiaoman Tian, Rui Ao, Xiangyu Long, Qiang Luo, Ping Duan, Jiang Zhu, Yongsheng Wang, Meijuan Huang, Yongmei Liu, Youling Gong","doi":"10.1007/s10637-024-01424-4","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with metastatic lung adenocarcinoma (MLA) and malignant pleural effusion (MPE) without driver gene mutations have a poor prognosis. None of the standard treatment strategies is recommended for such patients. We retrospectively analyzed the efficacy of the first-line treatment for this specific population: standard platinum-based doublet chemotherapy (CT), CT plus an immune checkpoint inhibitor (CT plus ICI), and CT plus bevacizumab (CT plus Bev). A total of 323 eligible patients were enrolled: CT alone (n = 166), CT plus Bev (n = 72), and CT plus ICI (n = 85). Treatment efficacy assessments were performed every two cycles according to the RECIST guidelines. The endpoints were overall survival (OS) and progression-free survival (PFS). Kaplan-Meier (K‒M) curves and the log-rank test were used to compare OS and PFS. p < 0.05 was the threshold of significance (statistical software: SPSS). The median follow-up was 11.4 months (range, 2.1-49.6 months). PFS and OS in the CT plus ICI/CT plus Bev cohort were significantly longer than those in the CT group (PFS: 7.8/6.4/3.9 months, p < 0.0001; OS: 16.4/15.6/9.6 months, p < 0.0001, respectively). CT plus Bev had better PFS and OS than CT plus ICI/CT in PD-L1 < 1% patients (PFS: 8.4/5.0/3.8 months, p < 0.0001; OS: 15.6/12.9/9.3 months, p < 0.0001). Among patients with PD-L1 1-49%, CT plus ICI led to a longer PFS and OS (PFS: 8.9/5.8/4.2 months, p = 0.009; OS: 24.2/18.8/11.5 months, p = 0.03). In the cohort with PD-L1 ≥ 50%, CT plus ICI was still the best first-line treatment (PFS: 19.7/13.8/9.6 months, p = 0.033; OS: 27.2/19.6/14.9 months, p = 0.047). In driver gene-negative MLA with MPE, CT plus Bev or ICI better controlled MPE and significantly prolonged survival compared to CT alone. PD-L1 expression (negative/positive) may be a key factor influencing the choice of CT plus Bev or ICI.</p>","PeriodicalId":14513,"journal":{"name":"Investigational New Drugs","volume":" ","pages":"196-206"},"PeriodicalIF":3.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10944392/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Investigational New Drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10637-024-01424-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
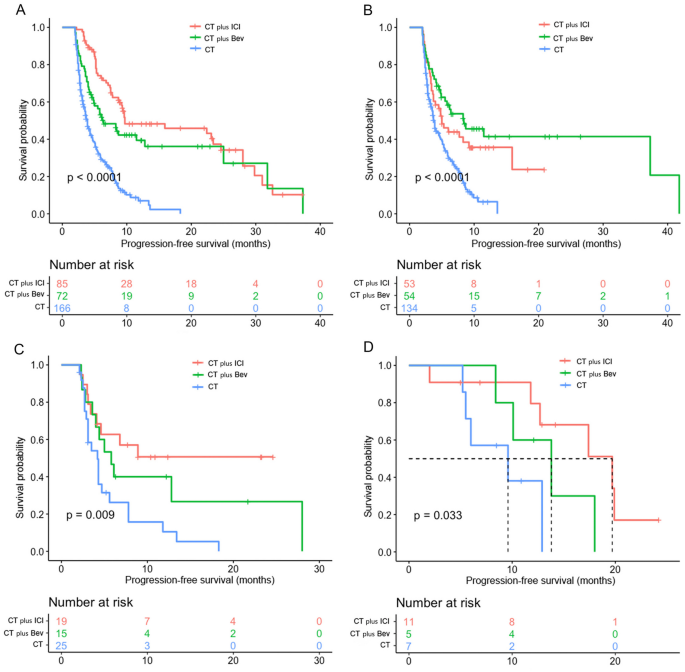
Patients with metastatic lung adenocarcinoma (MLA) and malignant pleural effusion (MPE) without driver gene mutations have a poor prognosis. None of the standard treatment strategies is recommended for such patients. We retrospectively analyzed the efficacy of the first-line treatment for this specific population: standard platinum-based doublet chemotherapy (CT), CT plus an immune checkpoint inhibitor (CT plus ICI), and CT plus bevacizumab (CT plus Bev). A total of 323 eligible patients were enrolled: CT alone (n = 166), CT plus Bev (n = 72), and CT plus ICI (n = 85). Treatment efficacy assessments were performed every two cycles according to the RECIST guidelines. The endpoints were overall survival (OS) and progression-free survival (PFS). Kaplan-Meier (K‒M) curves and the log-rank test were used to compare OS and PFS. p < 0.05 was the threshold of significance (statistical software: SPSS). The median follow-up was 11.4 months (range, 2.1-49.6 months). PFS and OS in the CT plus ICI/CT plus Bev cohort were significantly longer than those in the CT group (PFS: 7.8/6.4/3.9 months, p < 0.0001; OS: 16.4/15.6/9.6 months, p < 0.0001, respectively). CT plus Bev had better PFS and OS than CT plus ICI/CT in PD-L1 < 1% patients (PFS: 8.4/5.0/3.8 months, p < 0.0001; OS: 15.6/12.9/9.3 months, p < 0.0001). Among patients with PD-L1 1-49%, CT plus ICI led to a longer PFS and OS (PFS: 8.9/5.8/4.2 months, p = 0.009; OS: 24.2/18.8/11.5 months, p = 0.03). In the cohort with PD-L1 ≥ 50%, CT plus ICI was still the best first-line treatment (PFS: 19.7/13.8/9.6 months, p = 0.033; OS: 27.2/19.6/14.9 months, p = 0.047). In driver gene-negative MLA with MPE, CT plus Bev or ICI better controlled MPE and significantly prolonged survival compared to CT alone. PD-L1 expression (negative/positive) may be a key factor influencing the choice of CT plus Bev or ICI.
期刊介绍:
The development of new anticancer agents is one of the most rapidly changing aspects of cancer research. Investigational New Drugs provides a forum for the rapid dissemination of information on new anticancer agents. The papers published are of interest to the medical chemist, toxicologist, pharmacist, pharmacologist, biostatistician and clinical oncologist. Investigational New Drugs provides the fastest possible publication of new discoveries and results for the whole community of scientists developing anticancer agents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


