{"title":"Open Pancreatic Duct Stenting in Pancreatic Trauma: A Bridge in the Path of Pancreatic Preservation","authors":"Shardool Vikram Gupta, Apoorva Mardi, Srishti Bishnoi, Lalit Kumar Bansal, Achint Agarwal, Neeti Kapur","doi":"10.1007/s12262-024-04047-4","DOIUrl":null,"url":null,"abstract":"<p>Pancreatic trauma is often associated with high mortality and morbidity. Current management protocol advises conservative management when the duct is not involved but if there are higher-grade injuries with duct disruption it requires major pancreatic surgeries. These surgeries are technically challenging and carry a significant risk of morbidity and mortality. In this article, we propose open pancreatic duct stenting as the open counterpart of endoscopic retrograde cholangiopancreatography (ERCP) in open surgeries for pancreatic preservation. A 20-year-old male presented to emergency 3 days after blunt trauma abdomen with the chief complaint of upper abdominal pain and vomiting. Lab parameters were normal except <i>S. amylase</i> was − 1563 IU/L. Contrast-enhanced computerised tomography (CECT) abdomen shows almost complete transection at the level of the neck of the pancreas with complete disruption of the main pancreatic duct (MPD). Exploratory laparotomy with stenting of the pancreatic duct with pancreatic tissue repair with feeding jejunostomy was done instead of major pancreatic resection and anastomosis. The recovery period was uneventful, and the patient was discharged on the 8th postoperative day. In the literature, there are very few reports available where intraoperative pancreatic duct stenting was done without ductal repair in the trauma setting. Until now, ten cases have been reported in which a pancreatic duct could be approximated and was repaired over a stent. In recent years, there has been a paradigm shift in trauma management that advocates organ preservation. Existing pancreatic trauma guidelines still recommend morbid surgeries such as distal pancreatectomy or pancreaticoduodenectomy for severe-grade pancreatic trauma. However, there is an obvious need to consider organ preservation because pancreatic resection procedures have inherent complications as well as high morbidity and mortality.</p>","PeriodicalId":13391,"journal":{"name":"Indian Journal of Surgery","volume":"15 1","pages":""},"PeriodicalIF":0.4000,"publicationDate":"2024-02-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12262-024-04047-4","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
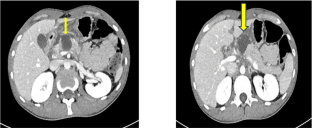
Pancreatic trauma is often associated with high mortality and morbidity. Current management protocol advises conservative management when the duct is not involved but if there are higher-grade injuries with duct disruption it requires major pancreatic surgeries. These surgeries are technically challenging and carry a significant risk of morbidity and mortality. In this article, we propose open pancreatic duct stenting as the open counterpart of endoscopic retrograde cholangiopancreatography (ERCP) in open surgeries for pancreatic preservation. A 20-year-old male presented to emergency 3 days after blunt trauma abdomen with the chief complaint of upper abdominal pain and vomiting. Lab parameters were normal except S. amylase was − 1563 IU/L. Contrast-enhanced computerised tomography (CECT) abdomen shows almost complete transection at the level of the neck of the pancreas with complete disruption of the main pancreatic duct (MPD). Exploratory laparotomy with stenting of the pancreatic duct with pancreatic tissue repair with feeding jejunostomy was done instead of major pancreatic resection and anastomosis. The recovery period was uneventful, and the patient was discharged on the 8th postoperative day. In the literature, there are very few reports available where intraoperative pancreatic duct stenting was done without ductal repair in the trauma setting. Until now, ten cases have been reported in which a pancreatic duct could be approximated and was repaired over a stent. In recent years, there has been a paradigm shift in trauma management that advocates organ preservation. Existing pancreatic trauma guidelines still recommend morbid surgeries such as distal pancreatectomy or pancreaticoduodenectomy for severe-grade pancreatic trauma. However, there is an obvious need to consider organ preservation because pancreatic resection procedures have inherent complications as well as high morbidity and mortality.
期刊介绍:
The Indian Journal of Surgery is the official publication of the Association of Surgeons of India that considers for publication articles in all fields of surgery. Issues are published bimonthly in the months of February, April, June, August, October and December.
The journal publishes Original article, Point of technique, Review article, Case report, Letter to editor, Teachers and surgeons from the past - A short (up to 500 words) bio sketch of a revered teacher or surgeon whom you hold in esteem and Images in surgery, surgical pathology, and surgical radiology.
A trusted resource for peer-reviewed coverage of all types of surgery
Provides a forum for surgeons in India and abroad to exchange ideas and advance the art of surgery
The official publication of the Association of Surgeons of India
92% of authors who answered a survey reported that they would definitely publish or probably publish in the journal again
The Indian Journal of Surgery offers peer-reviewed coverage of all types of surgery. The Journal publishes Original articles, Points of technique, Review articles, Case reports, Letters, Images and brief biographies of influential teachers and surgeons.
The Journal spans General Surgery, Pediatric Surgery, Neurosurgery, Plastic Surgery, Cardiothoracic Surgery, Vascular Surgery, Rural Surgery, Orthopedic Surgery, Urology, Surgical Oncology, Radiology, Anaesthesia, Trauma Services, Minimal Access Surgery, Endocrine Surgery, GI Surgery, ENT, Colorectal Surgery, surgical practice and research.
The Journal provides a forum for surgeons from India and abroad to exchange ideas, to propagate the advancement of science and the art of surgery and to promote friendship among surgeons in India and abroad. This has been a trusted platform for surgons in communicating up-to-date scientific informeation to the community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


