{"title":"Drug classes affecting intracranial aneurysm risk: Genetic correlation and Mendelian randomization.","authors":"Ynte M Ruigrok, Jan H Veldink, Mark K Bakker","doi":"10.1177/23969873241234134","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>There is no non-invasive treatment to prevent aneurysmal subarachnoid hemorrhage (ASAH) caused by intracranial aneurysm (IA) rupture. We aimed to identify drug classes that may affect liability to IA using a genetic approach.</p><p><strong>Patients and methods: </strong>Using genome-wide association summary statistics we calculated genetic correlation between unruptured IA (<i>N</i> = 2140 cases), ASAH (<i>N</i> = 5140) or the combined group, and liability to drug usage from 23 drug classes (<i>N</i> up to 320,000) independent of the risk factor high blood pressure. Next, we evaluated the causality and therapeutic potential of correlated drug classes using three different Mendelian randomization frameworks.</p><p><strong>Results: </strong>Correlations with IA were found for antidepressants, paracetamol, acetylsalicylic acid, opioids, beta-blockers, and peptic ulcer and gastro-esophageal reflux disease drugs. MR showed no evidence that genetically predicted usage of these drug classes caused IA. Genetically predicted high responders to antidepressant drugs were at higher risk of IA (odds ratio [OR] = 1.61, 95% confidence interval (CI) = 1.09-2.39, <i>p</i> = 0.018) and ASAH (OR = 1.68, 95% CI = 1.07-2.65, <i>p</i> = 0.024) if they used antidepressant drugs. This effect was absent in non-users. For beta-blockers, additional analyses showed that this effect was not independent of blood pressure after all. A complex and likely pleiotropic relationship was found between genetic liability to chronic multisite pain, pain medication usage (paracetamol, acetylsalicylic acid, and opioids), and IA.</p><p><strong>Conclusions: </strong>We did not find drugs decreasing liability to IA and ASAH but found that antidepressant drugs may increase liability. We observed pleiotropic relationships between IA and other drug classes and indications. Our results improve understanding of pathogenic mechanisms underlying IA.</p>","PeriodicalId":46821,"journal":{"name":"European Stroke Journal","volume":" ","pages":"687-695"},"PeriodicalIF":4.5000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11418413/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Stroke Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23969873241234134","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: There is no non-invasive treatment to prevent aneurysmal subarachnoid hemorrhage (ASAH) caused by intracranial aneurysm (IA) rupture. We aimed to identify drug classes that may affect liability to IA using a genetic approach.
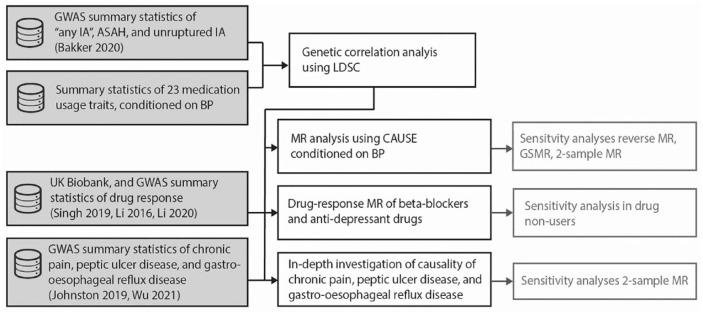
Patients and methods: Using genome-wide association summary statistics we calculated genetic correlation between unruptured IA (N = 2140 cases), ASAH (N = 5140) or the combined group, and liability to drug usage from 23 drug classes (N up to 320,000) independent of the risk factor high blood pressure. Next, we evaluated the causality and therapeutic potential of correlated drug classes using three different Mendelian randomization frameworks.
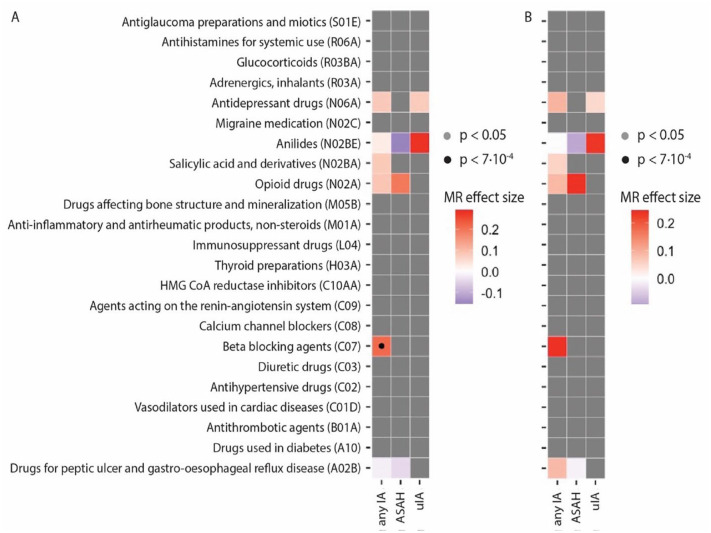
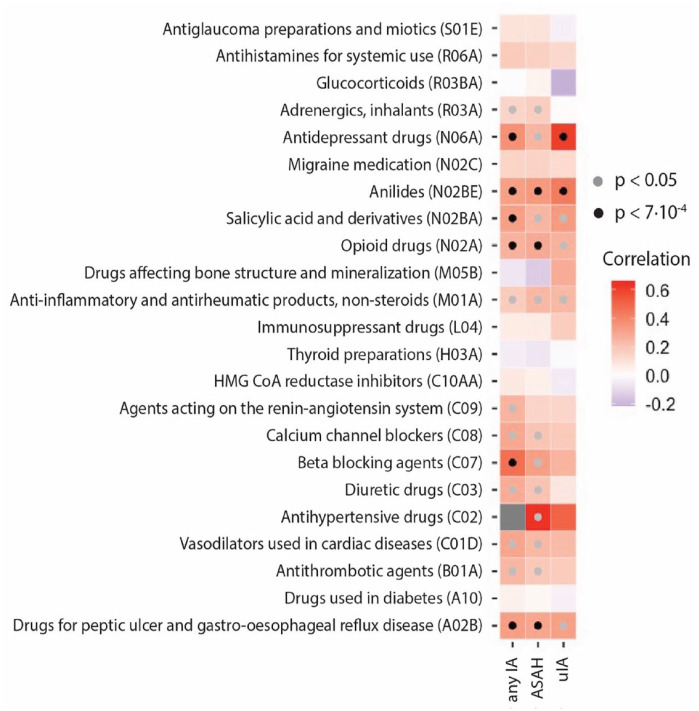
Results: Correlations with IA were found for antidepressants, paracetamol, acetylsalicylic acid, opioids, beta-blockers, and peptic ulcer and gastro-esophageal reflux disease drugs. MR showed no evidence that genetically predicted usage of these drug classes caused IA. Genetically predicted high responders to antidepressant drugs were at higher risk of IA (odds ratio [OR] = 1.61, 95% confidence interval (CI) = 1.09-2.39, p = 0.018) and ASAH (OR = 1.68, 95% CI = 1.07-2.65, p = 0.024) if they used antidepressant drugs. This effect was absent in non-users. For beta-blockers, additional analyses showed that this effect was not independent of blood pressure after all. A complex and likely pleiotropic relationship was found between genetic liability to chronic multisite pain, pain medication usage (paracetamol, acetylsalicylic acid, and opioids), and IA.
Conclusions: We did not find drugs decreasing liability to IA and ASAH but found that antidepressant drugs may increase liability. We observed pleiotropic relationships between IA and other drug classes and indications. Our results improve understanding of pathogenic mechanisms underlying IA.
期刊介绍:
Launched in 2016 the European Stroke Journal (ESJ) is the official journal of the European Stroke Organisation (ESO), a professional non-profit organization with over 1,400 individual members, and affiliations to numerous related national and international societies. ESJ covers clinical stroke research from all fields, including clinical trials, epidemiology, primary and secondary prevention, diagnosis, acute and post-acute management, guidelines, translation of experimental findings into clinical practice, rehabilitation, organisation of stroke care, and societal impact. It is open to authors from all relevant medical and health professions. Article types include review articles, original research, protocols, guidelines, editorials and letters to the Editor. Through ESJ, authors and researchers have gained a new platform for the rapid and professional publication of peer reviewed scientific material of the highest standards; publication in ESJ is highly competitive. The journal and its editorial team has developed excellent cooperation with sister organisations such as the World Stroke Organisation and the International Journal of Stroke, and the American Heart Organization/American Stroke Association and the journal Stroke. ESJ is fully peer-reviewed and is a member of the Committee on Publication Ethics (COPE). Issues are published 4 times a year (March, June, September and December) and articles are published OnlineFirst prior to issue publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


