{"title":"Antenatal diagnosis of congenital pouch colon: a case report from the Indian subcontinent with insights into management.","authors":"Jitendra Sharma, Rajesh Malik, Reyaz Ahmed","doi":"10.1093/bjrcr/uaad005","DOIUrl":null,"url":null,"abstract":"<p><p>Congenital pouch colon (CPC) is highly uncommon congenital anorectal malformation where a distended pouch-like structure replaces either some part of the colon or the entire colon and communicates to the genitourinary tract through a fistula. Diagnosis of CPC is usually made after birth when neonate/infant presents with abdominal distension and absence of anal opening. Making antenatal diagnosis of CPC is difficult because of the lack of specific and verifiable signs on sonography. Hence, only a few cases of antenatal diagnosis of CPC have been reported.<sup>1</sup><sup>,</sup><sup>2</sup> In our case, CPC was suspected on a routine antenatal growth scan ultrasound in the late third trimester, showing a hypoechoic tubular-shaped lesion in the pre-sacral region. With this suspicion, we suggested an institutional delivery at a tertiary level centre, and diagnosis of type III CPC was confirmed on post-delivery imaging and emergency primary surgery, done on the day 3 of life (pouch resection, division of fistula, and protective colostomy). The child also underwent further corrective surgeries in a staged manner in second year of life and recovered completely. Beforehand diagnosis prevented any unnecessary delay in operative care, reduced postoperative complications, and improved the overall outcome of this otherwise complex condition.</p>","PeriodicalId":45216,"journal":{"name":"BJR Case Reports","volume":"10 1","pages":"uaad005"},"PeriodicalIF":0.5000,"publicationDate":"2023-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10860509/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjrcr/uaad005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
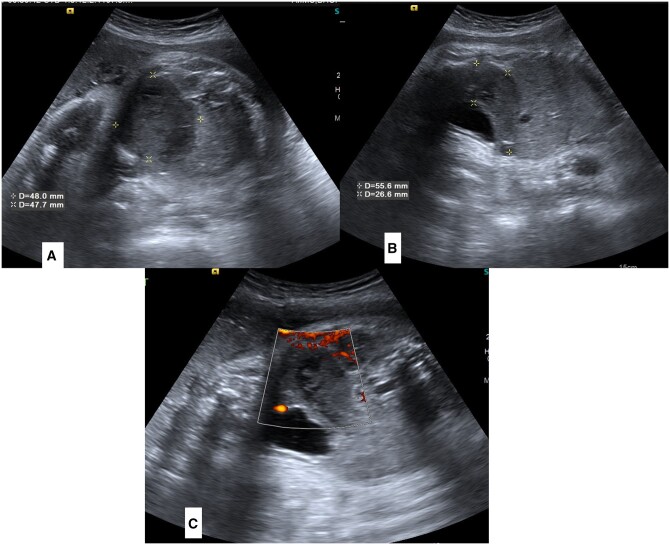
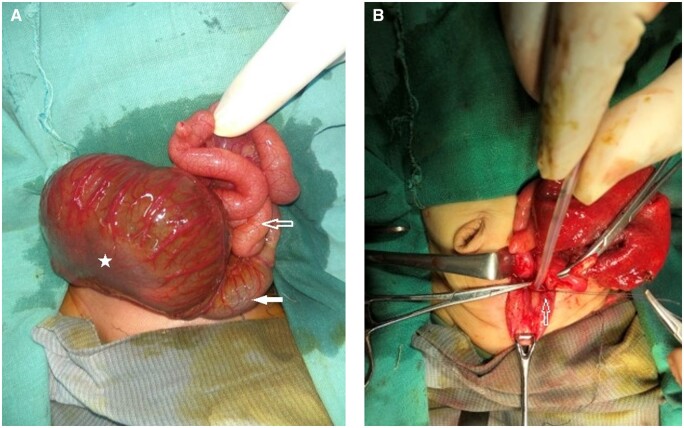
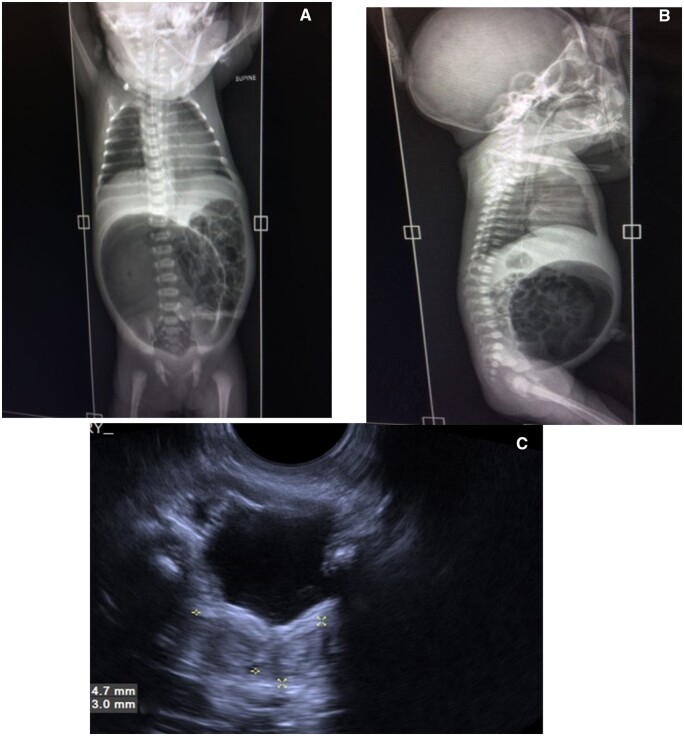
Congenital pouch colon (CPC) is highly uncommon congenital anorectal malformation where a distended pouch-like structure replaces either some part of the colon or the entire colon and communicates to the genitourinary tract through a fistula. Diagnosis of CPC is usually made after birth when neonate/infant presents with abdominal distension and absence of anal opening. Making antenatal diagnosis of CPC is difficult because of the lack of specific and verifiable signs on sonography. Hence, only a few cases of antenatal diagnosis of CPC have been reported.1,2 In our case, CPC was suspected on a routine antenatal growth scan ultrasound in the late third trimester, showing a hypoechoic tubular-shaped lesion in the pre-sacral region. With this suspicion, we suggested an institutional delivery at a tertiary level centre, and diagnosis of type III CPC was confirmed on post-delivery imaging and emergency primary surgery, done on the day 3 of life (pouch resection, division of fistula, and protective colostomy). The child also underwent further corrective surgeries in a staged manner in second year of life and recovered completely. Beforehand diagnosis prevented any unnecessary delay in operative care, reduced postoperative complications, and improved the overall outcome of this otherwise complex condition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


