David Oxborough, Danielle McDerment, Keith P George, Christopher Johnson, Barbara Morrison, Gemma Parry-Williams, Efstathios Papatheodorou, Sanjay Sharma, Robert Cooper
{"title":"Allometric scaling for left ventricular mass and geometry in male and female athletes of mixed and endurance sports.","authors":"David Oxborough, Danielle McDerment, Keith P George, Christopher Johnson, Barbara Morrison, Gemma Parry-Williams, Efstathios Papatheodorou, Sanjay Sharma, Robert Cooper","doi":"10.1186/s44156-024-00040-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The athlete's heart (AH) defines the phenotypical changes that occur in response to chronic exercise training. Echocardiographic assessment of the AH is used to calculate LV mass (LVM) and determine chamber geometry. This is, however, interpreted using standard linear (ratiometric) scaling to body surface area (BSA) whereas allometric scaling is now widely recommended. This study (1) determined whether ratiometric scaling of LVM to BSA (LVMi<sup>ratio</sup>) provides a size-independent index in young and veteran athletes of mixed and endurance sports (MES), and (2) calculated size-independent beta exponents for allometrically derived (LVMi<sup>allo</sup>) to BSA and (3) describes the physiological range of LVMi<sup>allo</sup> and the classifications of LV geometry.</p><p><strong>Methods: </strong>1373 MES athletes consisting of young (< 35 years old) (males n = 699 and females n = 127) and veteran (> 35 years old) (males n = 327 and females n = 220) were included in the study. LVMi<sup>ratio</sup> was calculated as per standard scaling and sex-specific LVMi<sup>allo</sup> were derived from the population. Cut-offs were defined and geometry was classified according to the new exponents and relative wall thickness.</p><p><strong>Results: </strong>LVMi<sup>ratio</sup> did not produce a size independent index. When tested across the age range the following indexes LVMi/BSA<sup>0.7663</sup> and LVMi/BSA<sup>0.52</sup>, for males and females respectively, were size independent (r = 0.012; P = 0.7 and r = 0.003; P = 0.920). Physiological cut-offs for LVMi<sup>allo</sup> were 135 g/(m<sup>2</sup>)<sup>0.7663</sup> in male athletes and 121 g/(m<sup>2</sup>)<sup>0.52</sup> in female athletes. Concentric remodelling / hypertrophy was present in 3% and 0% of young male and female athletes and 24% and 17% of veteran male and female athletes, respectively. Eccentric hypertrophy was observed in 8% and 6% of young male and female athletes and 9% and 11% of veteran male and female athletes, respectively.</p><p><strong>Conclusion: </strong>In a large cohort of young and veteran male and female MES athletes, LVMi<sup>ratio</sup> to BSA is not size independent. Sex-specific LVMi<sup>allo</sup> to BSA with LVMi/BSA<sup>0.77</sup> and LVMi/BSA<sup>0.52</sup> for male and female athletes respectively can be applied across the age-range. Population-based cut-offs of LVMi<sup>allo</sup> provided a physiological range demonstrating a predominance for normal geometry in all athlete groups with a greater percentage of concentric remodelling/hypertrophy occurring in veteran male and female athletes.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"11 1","pages":"4"},"PeriodicalIF":2.4000,"publicationDate":"2024-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10865516/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-024-00040-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The athlete's heart (AH) defines the phenotypical changes that occur in response to chronic exercise training. Echocardiographic assessment of the AH is used to calculate LV mass (LVM) and determine chamber geometry. This is, however, interpreted using standard linear (ratiometric) scaling to body surface area (BSA) whereas allometric scaling is now widely recommended. This study (1) determined whether ratiometric scaling of LVM to BSA (LVMiratio) provides a size-independent index in young and veteran athletes of mixed and endurance sports (MES), and (2) calculated size-independent beta exponents for allometrically derived (LVMiallo) to BSA and (3) describes the physiological range of LVMiallo and the classifications of LV geometry.
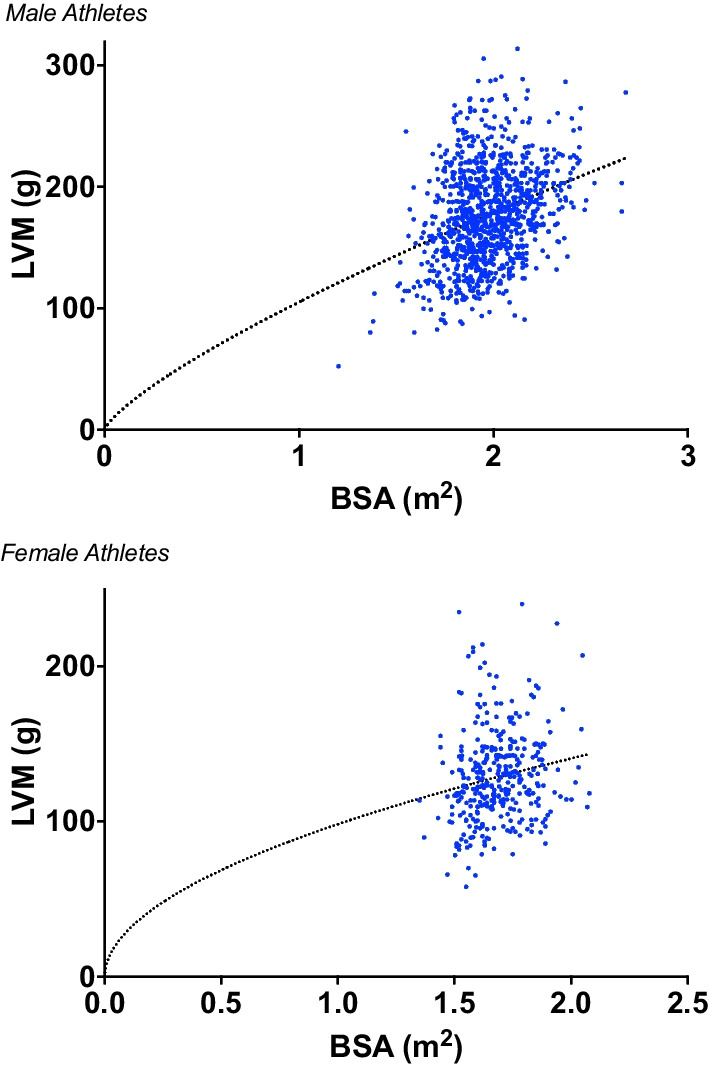
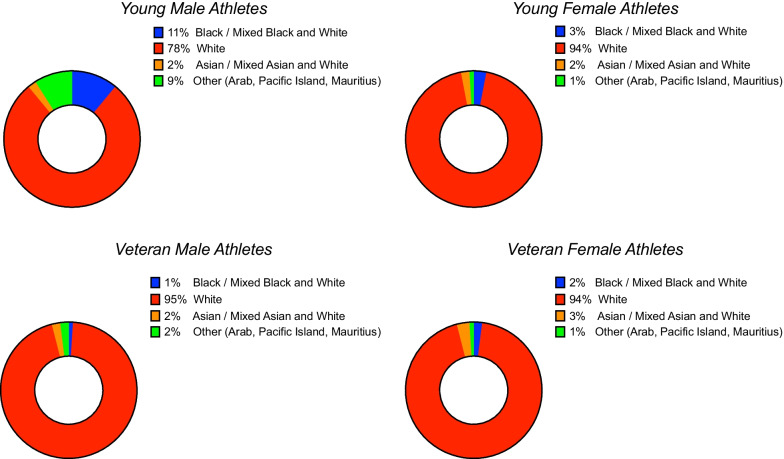
Methods: 1373 MES athletes consisting of young (< 35 years old) (males n = 699 and females n = 127) and veteran (> 35 years old) (males n = 327 and females n = 220) were included in the study. LVMiratio was calculated as per standard scaling and sex-specific LVMiallo were derived from the population. Cut-offs were defined and geometry was classified according to the new exponents and relative wall thickness.
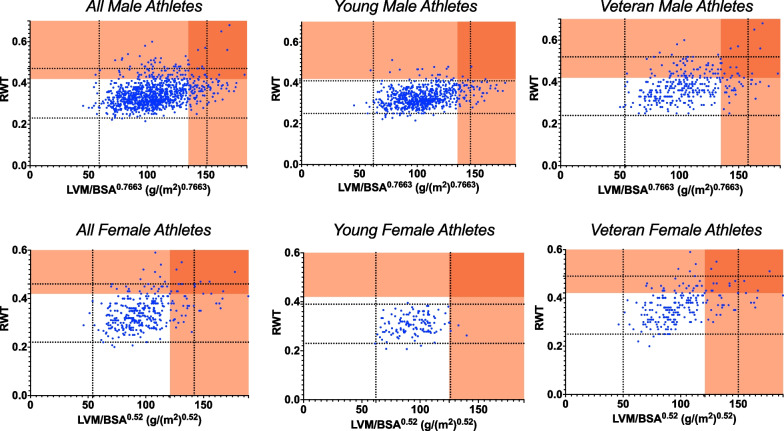
Results: LVMiratio did not produce a size independent index. When tested across the age range the following indexes LVMi/BSA0.7663 and LVMi/BSA0.52, for males and females respectively, were size independent (r = 0.012; P = 0.7 and r = 0.003; P = 0.920). Physiological cut-offs for LVMiallo were 135 g/(m2)0.7663 in male athletes and 121 g/(m2)0.52 in female athletes. Concentric remodelling / hypertrophy was present in 3% and 0% of young male and female athletes and 24% and 17% of veteran male and female athletes, respectively. Eccentric hypertrophy was observed in 8% and 6% of young male and female athletes and 9% and 11% of veteran male and female athletes, respectively.
Conclusion: In a large cohort of young and veteran male and female MES athletes, LVMiratio to BSA is not size independent. Sex-specific LVMiallo to BSA with LVMi/BSA0.77 and LVMi/BSA0.52 for male and female athletes respectively can be applied across the age-range. Population-based cut-offs of LVMiallo provided a physiological range demonstrating a predominance for normal geometry in all athlete groups with a greater percentage of concentric remodelling/hypertrophy occurring in veteran male and female athletes.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


