Joseph C Sweeney, Jaimin R Trivedi, Toyokazu Endo, Akhila Ankem, Siddharth V Pahwa, Mark S Slaughter, Brian L Ganzel
{"title":"Cannula Placement for Cerebral Protection Without Circulatory Arrest in Patients Undergoing Hemiarch Aortic Aneurysm Repair.","authors":"Joseph C Sweeney, Jaimin R Trivedi, Toyokazu Endo, Akhila Ankem, Siddharth V Pahwa, Mark S Slaughter, Brian L Ganzel","doi":"10.14503/THIJ-22-8026","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aortic aneurysms involving the proximal aortic arch, which require hemiarch-type repair, typically require circulatory arrest with antegrade cerebral perfusion. Left carotid antegrade cerebral perfusion (LCP) via distal arch cannulation without circulatory arrest was used in this study's patient population. The goal was to assess the operative efficiency and clinical outcomes of using a distal arch cannulation technique that would not require any hypothermic circulatory arrest (HCA) time compared with more traditional brachiocephalic artery cannulation with right-sided unilateral antegrade cerebral perfusion (RCP) and HCA.</p><p><strong>Methods: </strong>A single-center retrospective review of patients with replacement of the distal ascending aorta involving the proximal arch was performed. Patients with an intramural hematoma or dissection were excluded. Between January 2015 and December 2019, 68 adult patients had undergone a hemiarch repair because of aneurysmal disease. Analysis of baseline demographics, operative data, and clinical outcomes was performed.</p><p><strong>Results: </strong>Comparing the 68 patients: 21 patients were treated with RCP (via brachiocephalic artery graft with HCA), and 47 patients were treated with LCP (via distal aortic arch cannulation with cross-clamp between the brachiocephalic and left common carotid arteries without HCA). Baseline characteristics and outcomes were evaluated for both groups. The LCP group was younger (LCP median [IQR] age, 60 [53-65] years vs RCP median [IQR] age, 67 [59-71] years]. Sex, race, body mass index, comorbidities, and ejection fraction were similar between the groups. Cardiopulmonary bypass time (LCP, 123 minutes vs RCP, 149 minutes) and unilateral cerebral perfusion time (LCP, 17 minutes vs RCP, 22 minutes) were longer in the RCP group. Bleeding, prolonged ventilatory support, kidney failure, and length of stay were similar. In-hospital mortality was 2% in the LCP group vs 0% in the RCP group. Stroke occurred in 2 patients (4.2%) in the LCP group and in 0% of the RCP group. Mortality at 6 months in the LCP and RCP groups was 3% and 10%, respectively.</p><p><strong>Conclusion: </strong>Distal arch cannulation with LCP without HCA is a reasonable and safe alternative strategy for patients requiring hemiarch replacement for aneurysmal disease. This technique may provide additional benefits by avoiding circulatory arrest in these complex cases.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 1","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2024-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11075151/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-22-8026","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Aortic aneurysms involving the proximal aortic arch, which require hemiarch-type repair, typically require circulatory arrest with antegrade cerebral perfusion. Left carotid antegrade cerebral perfusion (LCP) via distal arch cannulation without circulatory arrest was used in this study's patient population. The goal was to assess the operative efficiency and clinical outcomes of using a distal arch cannulation technique that would not require any hypothermic circulatory arrest (HCA) time compared with more traditional brachiocephalic artery cannulation with right-sided unilateral antegrade cerebral perfusion (RCP) and HCA.
Methods: A single-center retrospective review of patients with replacement of the distal ascending aorta involving the proximal arch was performed. Patients with an intramural hematoma or dissection were excluded. Between January 2015 and December 2019, 68 adult patients had undergone a hemiarch repair because of aneurysmal disease. Analysis of baseline demographics, operative data, and clinical outcomes was performed.
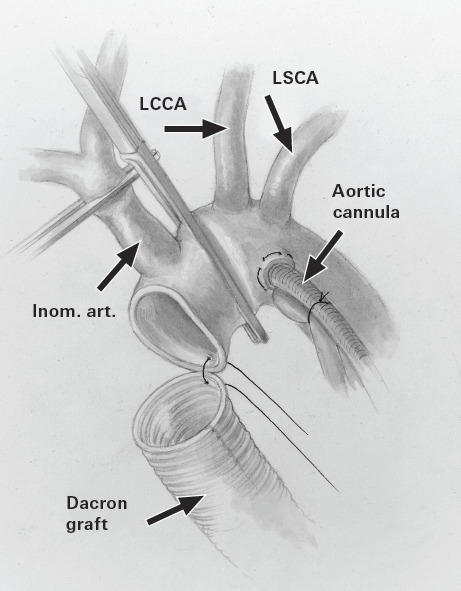
Results: Comparing the 68 patients: 21 patients were treated with RCP (via brachiocephalic artery graft with HCA), and 47 patients were treated with LCP (via distal aortic arch cannulation with cross-clamp between the brachiocephalic and left common carotid arteries without HCA). Baseline characteristics and outcomes were evaluated for both groups. The LCP group was younger (LCP median [IQR] age, 60 [53-65] years vs RCP median [IQR] age, 67 [59-71] years]. Sex, race, body mass index, comorbidities, and ejection fraction were similar between the groups. Cardiopulmonary bypass time (LCP, 123 minutes vs RCP, 149 minutes) and unilateral cerebral perfusion time (LCP, 17 minutes vs RCP, 22 minutes) were longer in the RCP group. Bleeding, prolonged ventilatory support, kidney failure, and length of stay were similar. In-hospital mortality was 2% in the LCP group vs 0% in the RCP group. Stroke occurred in 2 patients (4.2%) in the LCP group and in 0% of the RCP group. Mortality at 6 months in the LCP and RCP groups was 3% and 10%, respectively.
Conclusion: Distal arch cannulation with LCP without HCA is a reasonable and safe alternative strategy for patients requiring hemiarch replacement for aneurysmal disease. This technique may provide additional benefits by avoiding circulatory arrest in these complex cases.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


