Grace Guan, Neha S Joshi, Adam Frymoyer, Grace D Achepohl, Rebecca Dang, N Kenji Taylor, Joshua A Salomon, Jeremy D Goldhaber-Fiebert, Douglas K Owens
{"title":"Resource Utilization and Costs Associated with Approaches to Identify Infants with Early-Onset Sepsis.","authors":"Grace Guan, Neha S Joshi, Adam Frymoyer, Grace D Achepohl, Rebecca Dang, N Kenji Taylor, Joshua A Salomon, Jeremy D Goldhaber-Fiebert, Douglas K Owens","doi":"10.1177/23814683231226129","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective.</b> To compare resource utilization and costs associated with 3 alternative screening approaches to identify early-onset sepsis (EOS) in infants born at ≥35 wk of gestational age, as recommended by the American Academy of Pediatrics (AAP) in 2018. <b>Study Design.</b> Decision tree-based cost analysis of the 3 AAP-recommended approaches: 1) categorical risk assessment (categorization by chorioamnionitis exposure status), 2) neonatal sepsis calculator (a multivariate prediction model based on perinatal risk factors), and 3) enhanced clinical observation (assessment based on serial clinical examinations). We evaluated resource utilization and direct costs (2022 US dollars) to the health system. <b>Results.</b> Categorical risk assessment led to the greatest neonatal intensive care unit usage (210 d per 1,000 live births) and antibiotic exposure (6.8%) compared with the neonatal sepsis calculator (112 d per 1,000 live births and 3.6%) and enhanced clinical observation (99 d per 1,000 live births and 3.1%). While the per-live birth hospital costs of the 3 approaches were similar-categorical risk assessment cost $1,360, the neonatal sepsis calculator cost $1,317, and enhanced clinical observation cost $1,310-the cost of infants receiving intervention under categorical risk assessment was approximately twice that of the other 2 strategies. Results were robust to variations in data parameters. <b>Conclusion.</b> The neonatal sepsis calculator and enhanced clinical observation approaches may be preferred to categorical risk assessment as they reduce the number of infants receiving intervention and thus antibiotic exposure and associated costs. All 3 approaches have similar costs over all live births, and prior literature has indicated similar health outcomes. Inclusion of downstream effects of antibiotic exposure in the neonatal period should be evaluated within a cost-effectiveness analysis.</p><p><strong>Highlights: </strong>Of the 3 approaches recommended by the American Academy of Pediatrics in 2018 to identify early-onset sepsis in infants born at ≥35 weeks, the categorical risk assessment approach leads to about twice as many infants receiving evaluation to rule out early-onset sepsis compared with the neonatal sepsis calculator and enhanced clinical observation approaches.While the hospital costs of the 3 approaches were similar over the entire population of live births, the neonatal sepsis calculator and enhanced clinical observation approaches reduce antibiotic exposure, neonatal intensive care unit admission, and hospital costs associated with interventions as part of the screening approach compared with the categorical risk assessment approach.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"9 1","pages":"23814683231226129"},"PeriodicalIF":1.7000,"publicationDate":"2024-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10826394/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683231226129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
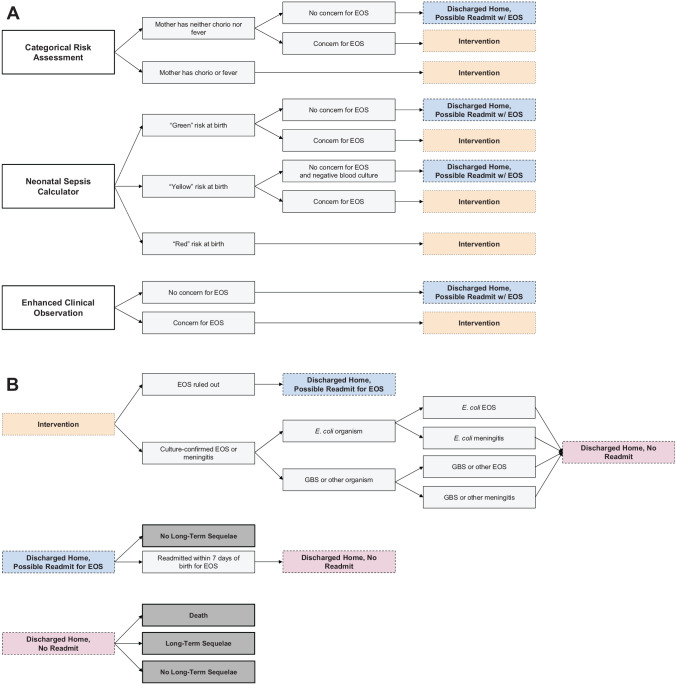
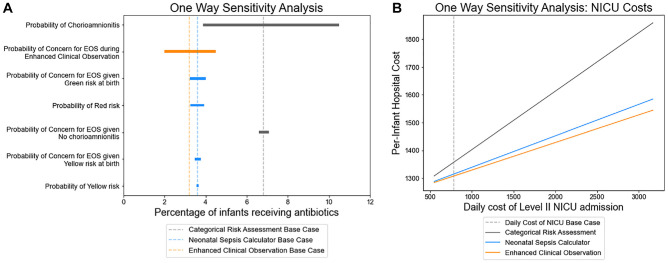
Objective. To compare resource utilization and costs associated with 3 alternative screening approaches to identify early-onset sepsis (EOS) in infants born at ≥35 wk of gestational age, as recommended by the American Academy of Pediatrics (AAP) in 2018. Study Design. Decision tree-based cost analysis of the 3 AAP-recommended approaches: 1) categorical risk assessment (categorization by chorioamnionitis exposure status), 2) neonatal sepsis calculator (a multivariate prediction model based on perinatal risk factors), and 3) enhanced clinical observation (assessment based on serial clinical examinations). We evaluated resource utilization and direct costs (2022 US dollars) to the health system. Results. Categorical risk assessment led to the greatest neonatal intensive care unit usage (210 d per 1,000 live births) and antibiotic exposure (6.8%) compared with the neonatal sepsis calculator (112 d per 1,000 live births and 3.6%) and enhanced clinical observation (99 d per 1,000 live births and 3.1%). While the per-live birth hospital costs of the 3 approaches were similar-categorical risk assessment cost $1,360, the neonatal sepsis calculator cost $1,317, and enhanced clinical observation cost $1,310-the cost of infants receiving intervention under categorical risk assessment was approximately twice that of the other 2 strategies. Results were robust to variations in data parameters. Conclusion. The neonatal sepsis calculator and enhanced clinical observation approaches may be preferred to categorical risk assessment as they reduce the number of infants receiving intervention and thus antibiotic exposure and associated costs. All 3 approaches have similar costs over all live births, and prior literature has indicated similar health outcomes. Inclusion of downstream effects of antibiotic exposure in the neonatal period should be evaluated within a cost-effectiveness analysis.
Highlights: Of the 3 approaches recommended by the American Academy of Pediatrics in 2018 to identify early-onset sepsis in infants born at ≥35 weeks, the categorical risk assessment approach leads to about twice as many infants receiving evaluation to rule out early-onset sepsis compared with the neonatal sepsis calculator and enhanced clinical observation approaches.While the hospital costs of the 3 approaches were similar over the entire population of live births, the neonatal sepsis calculator and enhanced clinical observation approaches reduce antibiotic exposure, neonatal intensive care unit admission, and hospital costs associated with interventions as part of the screening approach compared with the categorical risk assessment approach.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


