Sukyo Lee, Sungjin Kim, Sejoong Ahn, Hanjin Cho, Sungwoo Moon, Young Duck Cho, Jong-Hak Park
{"title":"The mortality of patients with sepsis increases in the first month of a new academic year.","authors":"Sukyo Lee, Sungjin Kim, Sejoong Ahn, Hanjin Cho, Sungwoo Moon, Young Duck Cho, Jong-Hak Park","doi":"10.15441/ceem.23.117","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Many studies have examined the July effect. However, little is known about the July effect in sepsis. We hypothesized that the July effect would result in worse outcomes for patients with sepsis.</p><p><strong>Methods: </strong>Data from patients with sepsis, collected prospectively between January 2018 and December 2021, were analyzed. In Korea, the new academic year starts on March 1, so the \"July effect\" appears in March. The primary outcome was 30-day mortality. Secondary outcomes included adherence to the Surviving Sepsis Campaign bundle. Outcomes in March were compared to other months. A multivariate Cox proportional hazard regression was performed to adjust for confounders.</p><p><strong>Results: </strong>We included 843 patients. There were no significant differences in sepsis severity. The 30-day mortality in March was higher (49.0% vs. 28.5%, P<0.001). However, there was no difference in bundle adherence in March (42.2% vs. 48.0%, P=0.264). The multivariate Cox proportional hazard regression showed that the July effect was associated with 30-day mortality in patients with sepsis (adjusted hazard ratio, 1.925; 95% confidence interval, 1.405-2.638; P<0.001).</p><p><strong>Conclusion: </strong>The July effect was associated with 30-day mortality in patients with sepsis. However, bundle adherence did not differ. These.</p><p><strong>Results: </strong>suggest that the increase in mortality during the turnover period might be related to unmeasured in-hospital management. Intensive supervision and education of residents caring for patients with sepsis is needed in the beginning of training.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"161-170"},"PeriodicalIF":2.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11237255/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.23.117","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Many studies have examined the July effect. However, little is known about the July effect in sepsis. We hypothesized that the July effect would result in worse outcomes for patients with sepsis.
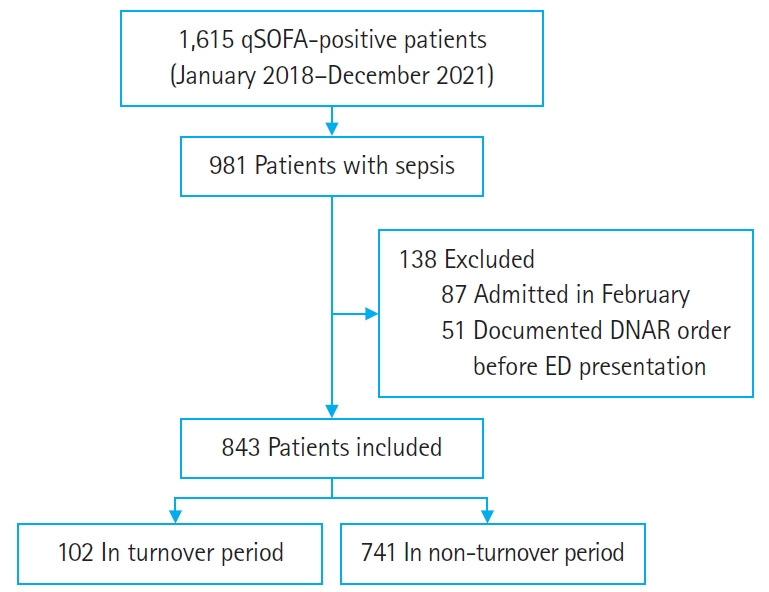
Methods: Data from patients with sepsis, collected prospectively between January 2018 and December 2021, were analyzed. In Korea, the new academic year starts on March 1, so the "July effect" appears in March. The primary outcome was 30-day mortality. Secondary outcomes included adherence to the Surviving Sepsis Campaign bundle. Outcomes in March were compared to other months. A multivariate Cox proportional hazard regression was performed to adjust for confounders.
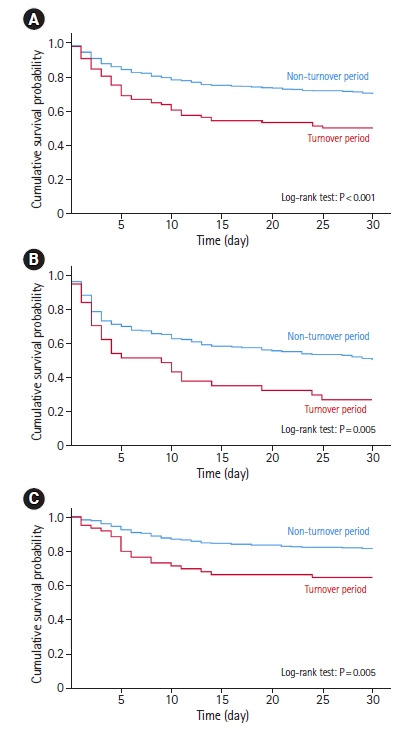
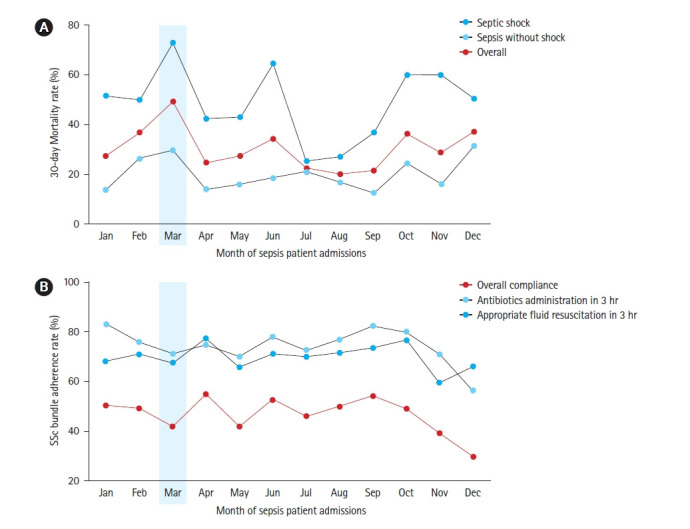
Results: We included 843 patients. There were no significant differences in sepsis severity. The 30-day mortality in March was higher (49.0% vs. 28.5%, P<0.001). However, there was no difference in bundle adherence in March (42.2% vs. 48.0%, P=0.264). The multivariate Cox proportional hazard regression showed that the July effect was associated with 30-day mortality in patients with sepsis (adjusted hazard ratio, 1.925; 95% confidence interval, 1.405-2.638; P<0.001).
Conclusion: The July effect was associated with 30-day mortality in patients with sepsis. However, bundle adherence did not differ. These.
Results: suggest that the increase in mortality during the turnover period might be related to unmeasured in-hospital management. Intensive supervision and education of residents caring for patients with sepsis is needed in the beginning of training.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


