Enrica Antonia Martino, Francesca Romana Mauro, Gianluigi Reda, Luca Laurenti, Andrea Visentin, Annamaria Frustaci, Ernesto Vigna, Sara Pepe, Gioacchino Catania, Giacomo Loseto, Roberta Murru, Annalisa Chiarenza, Paolo Sportoletti, Maria Ilaria Del Principe, Roberta Laureana, Marta Coscia, Sara Galimberti, Eleonora Ferretti, Antonella Zucchetto, Riccardo Bomben, Jerry Polesel, Alessandra Tedeschi, Davide Rossi, Livio Trentin, Antonino Neri, Fortunato Morabito, Valter Gattei, Massimo Gentile
{"title":"Ibrutinib as first line therapy in chronic lymphocytic leukemia patients over 80 years old: A retrospective real-life multicenter Italian cohort","authors":"Enrica Antonia Martino, Francesca Romana Mauro, Gianluigi Reda, Luca Laurenti, Andrea Visentin, Annamaria Frustaci, Ernesto Vigna, Sara Pepe, Gioacchino Catania, Giacomo Loseto, Roberta Murru, Annalisa Chiarenza, Paolo Sportoletti, Maria Ilaria Del Principe, Roberta Laureana, Marta Coscia, Sara Galimberti, Eleonora Ferretti, Antonella Zucchetto, Riccardo Bomben, Jerry Polesel, Alessandra Tedeschi, Davide Rossi, Livio Trentin, Antonino Neri, Fortunato Morabito, Valter Gattei, Massimo Gentile","doi":"10.1002/hon.3249","DOIUrl":null,"url":null,"abstract":"<p>Although chronic lymphocytic leukemia (CLL) predominantly affects the elderly, limited data exists about the outcomes of over 80-year-old patients, usually underrepresented in clinical trials. We conducted a multicenter study enrolling 79 consecutive CLL patients ≥80 years at the time of frontline therapy, all treated with ibrutinib. Nearly 48% of cases exhibited unmutated <i>IGHV</i> genes, 32% 17p deletion, and 39.2% <i>TP53</i> mutations; 63.3% displayed a cumulative illness rating scale (CIRS) > 6. The overall response rate on ibrutinib, computed in 74/79 patients (5 patients excluded for early withdrawal), was 89.9%. After a median follow-up of 28.9 months, the median progression-free survival (PFS) and overall survival (OS) were 42.5 and 51.8 months, respectively. CIRS>6 and temporary discontinuation of ibrutinib lasting for 7–30 days were the only parameters associated with a significantly shorter PFS and were both relevant in predicting a shorter PFS compared to patients with CIRS≤6 and therapy discontinuation ≤7 days. The most common grade≥3 adverse events were infections (25.5%), neutropenia (10.1%), and anemia (2.5%). Eighteen patients (22.8%) experienced a cardiovascular event, including grade-2 atrial fibrillation (<i>n</i> = 9; 11%), grade-2 hypertension (<i>n</i> = 5; 6%), heart failure (<i>n</i> = 3; 3%), and acute coronary syndrome (<i>n</i> = 1; 1%). Mild bleeding events were observed in 27 patients (34.2%). Ibrutinib was permanently discontinued in 26 patients due to progressive disease (<i>n</i> = 11, including 5 Richter's syndromes), secondary malignancies (<i>n</i> = 6), infections (<i>n</i> = 3), cardiac failure (<i>n</i> = 3), severe bleeding (<i>n</i> = 2), and sudden death (<i>n</i> = 1). In conclusion, our analyses confirmed the overall effectiveness and favorable safety profile of the ibrutinib-single agent therapeutic approach in CLL patients ≥80 years.</p>","PeriodicalId":12882,"journal":{"name":"Hematological Oncology","volume":"42 1","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2024-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3249","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematological Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hon.3249","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
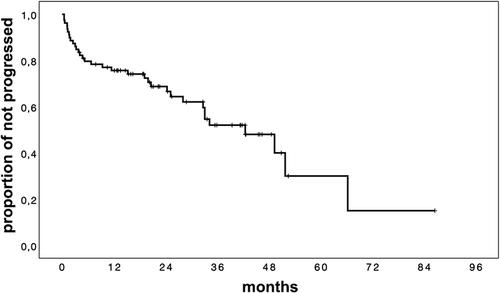
Although chronic lymphocytic leukemia (CLL) predominantly affects the elderly, limited data exists about the outcomes of over 80-year-old patients, usually underrepresented in clinical trials. We conducted a multicenter study enrolling 79 consecutive CLL patients ≥80 years at the time of frontline therapy, all treated with ibrutinib. Nearly 48% of cases exhibited unmutated IGHV genes, 32% 17p deletion, and 39.2% TP53 mutations; 63.3% displayed a cumulative illness rating scale (CIRS) > 6. The overall response rate on ibrutinib, computed in 74/79 patients (5 patients excluded for early withdrawal), was 89.9%. After a median follow-up of 28.9 months, the median progression-free survival (PFS) and overall survival (OS) were 42.5 and 51.8 months, respectively. CIRS>6 and temporary discontinuation of ibrutinib lasting for 7–30 days were the only parameters associated with a significantly shorter PFS and were both relevant in predicting a shorter PFS compared to patients with CIRS≤6 and therapy discontinuation ≤7 days. The most common grade≥3 adverse events were infections (25.5%), neutropenia (10.1%), and anemia (2.5%). Eighteen patients (22.8%) experienced a cardiovascular event, including grade-2 atrial fibrillation (n = 9; 11%), grade-2 hypertension (n = 5; 6%), heart failure (n = 3; 3%), and acute coronary syndrome (n = 1; 1%). Mild bleeding events were observed in 27 patients (34.2%). Ibrutinib was permanently discontinued in 26 patients due to progressive disease (n = 11, including 5 Richter's syndromes), secondary malignancies (n = 6), infections (n = 3), cardiac failure (n = 3), severe bleeding (n = 2), and sudden death (n = 1). In conclusion, our analyses confirmed the overall effectiveness and favorable safety profile of the ibrutinib-single agent therapeutic approach in CLL patients ≥80 years.
期刊介绍:
Hematological Oncology considers for publication articles dealing with experimental and clinical aspects of neoplastic diseases of the hemopoietic and lymphoid systems and relevant related matters. Translational studies applying basic science to clinical issues are particularly welcomed. Manuscripts dealing with the following areas are encouraged:
-Clinical practice and management of hematological neoplasia, including: acute and chronic leukemias, malignant lymphomas, myeloproliferative disorders
-Diagnostic investigations, including imaging and laboratory assays
-Epidemiology, pathology and pathobiology of hematological neoplasia of hematological diseases
-Therapeutic issues including Phase 1, 2 or 3 trials as well as allogeneic and autologous stem cell transplantation studies
-Aspects of the cell biology, molecular biology, molecular genetics and cytogenetics of normal or diseased hematopoeisis and lymphopoiesis, including stem cells and cytokines and other regulatory systems.
Concise, topical review material is welcomed, especially if it makes new concepts and ideas accessible to a wider community. Proposals for review material may be discussed with the Editor-in-Chief. Collections of case material and case reports will be considered only if they have broader scientific or clinical relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


