Joseph F. Zywiciel BS , Raymond A. Verm MD , Wissam Raad MD , Marshall Baker MD, FACS , Richard Freeman MD, MBA , Zaid M. Abdelsattar MD, MS, FACS
{"title":"En bloc chest wall resection in locally advanced cT3N2 (stage IIIB) lung cancer involving the chest wall: Revisiting guidelines","authors":"Joseph F. Zywiciel BS , Raymond A. Verm MD , Wissam Raad MD , Marshall Baker MD, FACS , Richard Freeman MD, MBA , Zaid M. Abdelsattar MD, MS, FACS","doi":"10.1016/j.xjon.2023.12.007","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>Current National Comprehensive Cancer Network guidelines recommend definitive chemoradiation rather than surgery for patients with locally advanced clinical stage T3 and N2 (stage IIIB) lung cancer involving the chest wall. The data supporting this recommendation are controversial. We studied whether surgery confers a survival advantage over definitive chemoradiation in the National Cancer Database.</p></div><div><h3>Methods</h3><p>We identified all patients with clinical stage T3 and N2 lung cancer in the National Cancer Database from 2004 to 2017 who underwent a lobectomy with en bloc chest wall resection and compared them with patients with clinical stage T3 and N2 lung cancer who had definitive chemoradiation. We used propensity score matching to minimize confounding by indication while excluding patients with tumors in the upper lobes to exclude Pancoast tumors. We used 1:1 propensity score matching and Kaplan–Meir survival analyses to estimate associations.</p></div><div><h3>Results</h3><p>Of 4467 patients meeting all inclusion/exclusion criteria, 210 (4.49%) had an en bloc chest wall resection. Patients undergoing surgical resection were younger (mean age = 60.3 ± 10.3 years vs 67.5 ± 10.4 years; <em>P</em> < .001) and had more adenocarcinoma (59.0% vs 44.5%; <em>P</em> < .001) but were otherwise similar in terms of sex (37.1% female vs 42.0%; <em>P</em> = .167) and race (Whites 84.3% vs 84.0%; <em>P</em> = .276) compared with the definitive chemoradiation group. After resection, there was an unadjusted 30- and 90-day mortality rate of 3.3% and 9.5%, respectively. A substantial survival benefit with surgical resection persisted after propensity score matching (log-rank <em>P</em> < .001).</p></div><div><h3>Conclusions</h3><p>In this large observational study, we found that in select patients, en bloc chest wall resection for locally advanced clinical stage T3 and N2 lung cancer was associated with improved survival compared with definitive chemoradiation. National Comprehensive Cancer Network guidelines should be revisited.</p></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666273623004242/pdfft?md5=3293b1306bd400e9ba025f2cadfbe7ce&pid=1-s2.0-S2666273623004242-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273623004242","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
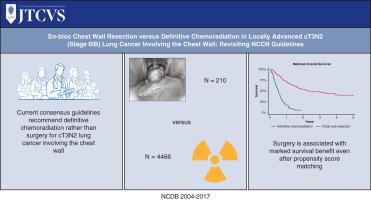
Current National Comprehensive Cancer Network guidelines recommend definitive chemoradiation rather than surgery for patients with locally advanced clinical stage T3 and N2 (stage IIIB) lung cancer involving the chest wall. The data supporting this recommendation are controversial. We studied whether surgery confers a survival advantage over definitive chemoradiation in the National Cancer Database.
Methods
We identified all patients with clinical stage T3 and N2 lung cancer in the National Cancer Database from 2004 to 2017 who underwent a lobectomy with en bloc chest wall resection and compared them with patients with clinical stage T3 and N2 lung cancer who had definitive chemoradiation. We used propensity score matching to minimize confounding by indication while excluding patients with tumors in the upper lobes to exclude Pancoast tumors. We used 1:1 propensity score matching and Kaplan–Meir survival analyses to estimate associations.
Results
Of 4467 patients meeting all inclusion/exclusion criteria, 210 (4.49%) had an en bloc chest wall resection. Patients undergoing surgical resection were younger (mean age = 60.3 ± 10.3 years vs 67.5 ± 10.4 years; P < .001) and had more adenocarcinoma (59.0% vs 44.5%; P < .001) but were otherwise similar in terms of sex (37.1% female vs 42.0%; P = .167) and race (Whites 84.3% vs 84.0%; P = .276) compared with the definitive chemoradiation group. After resection, there was an unadjusted 30- and 90-day mortality rate of 3.3% and 9.5%, respectively. A substantial survival benefit with surgical resection persisted after propensity score matching (log-rank P < .001).
Conclusions
In this large observational study, we found that in select patients, en bloc chest wall resection for locally advanced clinical stage T3 and N2 lung cancer was associated with improved survival compared with definitive chemoradiation. National Comprehensive Cancer Network guidelines should be revisited.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


