Concomitant presentation of thrombotic thrombocytopenic purpura, immune thrombocytopenia, and autoimmune hemolytic anemia in a patient with newly diagnosed systemic lupus erythematosus.
Lina Bruns, Linus Völker, Robert Klamroth, Martin K Kuhlmann, Wolfram J Jabs
{"title":"Concomitant presentation of thrombotic thrombocytopenic purpura, immune thrombocytopenia, and autoimmune hemolytic anemia in a patient with newly diagnosed systemic lupus erythematosus.","authors":"Lina Bruns, Linus Völker, Robert Klamroth, Martin K Kuhlmann, Wolfram J Jabs","doi":"10.5414/CNCS111193","DOIUrl":null,"url":null,"abstract":"<p><p>Thrombocytopenia is always of concern when encountered in emergency settings. We report a case of a 29-year-old women in whom a unique constellation of hematological disorders occurred. The patient had been diagnosed with idiopathic immune thrombocytopenia (ITP) in 2007, with a history of several thrombocytopenic flares. She now presented with homonymous hemianopia accompanied by thrombocytopenia and microangiopathic hemolytic anemia (MAHA) and was soon after diagnosed with a posterior stroke. Symptoms were more reminiscent of acquired thrombotic thrombocytopenic purpura (aTTP) rather than ITP. Immediate treatment with plasma exchange and caplacizumab curtailed MAHA, and progressive ischemic disease was averted. ADAMTS-13 testing confirmed the diagnosis of immune-mediated aTTP. Repeated testing for ITP, however, also showed IgG-loaded thrombocytes with the former known anti-GPIIb/IIIa specificity. Furthermore, autoimmune hemolytic anemia (AIHA) could be detected by direct antiglobulin test showing IgG and complement loading of the patient's erythrocytes. The autoimmune background of all three entities suggested an underlying systemic disease. Indeed, systemic lupus erythematosus (SLE) serology was strongly positive allowing for the diagnosis of SLE. ITP and AIHA as well as aTTP can be secondary to SLE, but emergence of all three disorders has not been reported at the same time.</p>","PeriodicalId":510898,"journal":{"name":"Clinical nephrology. Case studies","volume":"11 ","pages":"147-153"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10759207/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical nephrology. Case studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS111193","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
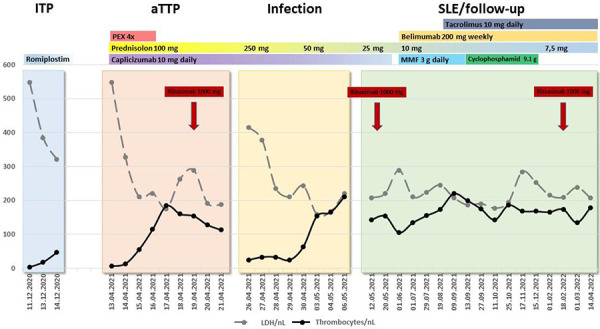
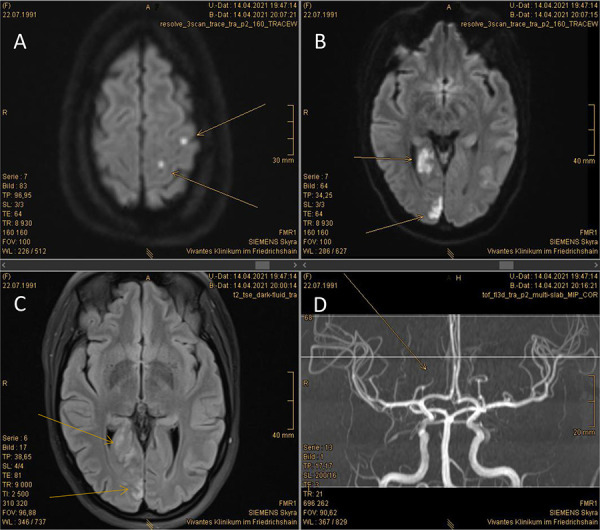
Thrombocytopenia is always of concern when encountered in emergency settings. We report a case of a 29-year-old women in whom a unique constellation of hematological disorders occurred. The patient had been diagnosed with idiopathic immune thrombocytopenia (ITP) in 2007, with a history of several thrombocytopenic flares. She now presented with homonymous hemianopia accompanied by thrombocytopenia and microangiopathic hemolytic anemia (MAHA) and was soon after diagnosed with a posterior stroke. Symptoms were more reminiscent of acquired thrombotic thrombocytopenic purpura (aTTP) rather than ITP. Immediate treatment with plasma exchange and caplacizumab curtailed MAHA, and progressive ischemic disease was averted. ADAMTS-13 testing confirmed the diagnosis of immune-mediated aTTP. Repeated testing for ITP, however, also showed IgG-loaded thrombocytes with the former known anti-GPIIb/IIIa specificity. Furthermore, autoimmune hemolytic anemia (AIHA) could be detected by direct antiglobulin test showing IgG and complement loading of the patient's erythrocytes. The autoimmune background of all three entities suggested an underlying systemic disease. Indeed, systemic lupus erythematosus (SLE) serology was strongly positive allowing for the diagnosis of SLE. ITP and AIHA as well as aTTP can be secondary to SLE, but emergence of all three disorders has not been reported at the same time.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


