Effects of rurality and distance to care on perinatal outcomes over a 1-year period during the COVID-19 pandemic
Abstract
Purpose
Our aim was to investigate the roles of rurality and distance to care on adverse perinatal outcomes and COVID-19 seroprevalence at the time of delivery over a 1-year period.
Methods
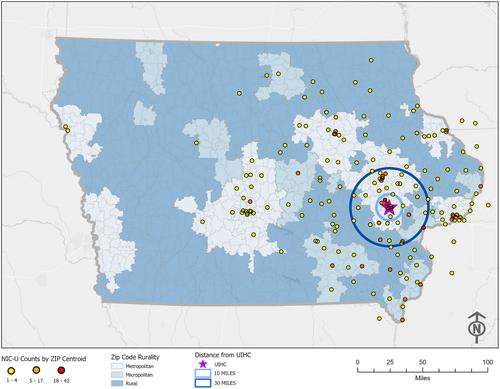
Data were collected from the electronic medical record on all pregnant patients who delivered at a single, large, Midwest academic medical center over 1 year. Rurality was classified using standard Rural-Urban Commuting Area codes. Geographic Information System tools were used to map outcomes. Data were analyzed with univariate and multivariate models, controlling for Body Mass Index (BMI), insurance status, and parity.
Findings
A total of 2,497 patients delivered during the study period; 20% of patients were rural (n = 499), 18.6% were micropolitan (n = 466), and 61.4% were metropolitan (n = 1,532). 10.4% of patients (n = 259) were COVID-19 seropositive. Rural patients did not experience higher rates of any measured adverse outcomes than metropolitan patients; micropolitan patients had increased odds of preterm labor (OR = 1.41, P = .022) and pre-eclampsia (OR = 1.78, P<.001). Patients living 30+ miles away from the medical center had increased odds of preterm labor (OR = 1.94, P<.001), pre-eclampsia (OR = 1.73, P = .002), and infant admission to the neonatal intensive care unit (OR = 2.12, P<.001), as well as lower gestational age at delivery (β = −9.2 days, P<.001) and birth weight (β = −206 grams, P<.001).
Conclusion
Distance to care, rather than rurality, was the key predictor of multiple adverse perinatal outcomes in this cohort of deliveries over a 1-year period. Our study suggests that rurality should not be used as a standalone indicator of access to care without further knowledge of the specific barriers affecting a given population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


