{"title":"Challenges of treating catatonia in the community setting without access to electroconvulsive therapy.","authors":"Tyler Torrico, Shahzeb Shaheen, David Weinstein, Ranjit Padhy, Md Towhid Salam","doi":"10.1177/27550834231220504","DOIUrl":null,"url":null,"abstract":"<p><p>Catatonia is a psychomotor syndrome resulting from an underlying psychiatric or medical disorder commonly observed in inpatient psychiatric units. While benzodiazepines and electroconvulsive therapy (ECT) are effective treatment options, the unavailability of ECT in many community psychiatric hospitals in the United States negatively affects patient outcomes. We present a 25-year-old African American male with a psychiatric diagnosis of schizophrenia complicated by malignant catatonia who was admitted to a community psychiatric hospital. He required intensive medical stabilization with supportive management, and transfer requests to ECT-equipped hospitals were initiated. While awaiting transfer for 148 days, the patient's symptoms did not fully remit with lorazepam (even with 36 mg daily in divided doses) and other psychotropic medication trials, including antipsychotics and mood stabilizers. After nearly 5 months of inpatient stay, he was successfully transferred, received ECT treatment, and experienced rapid resolution of catatonia. After discharge, to obtain three monthly sessions of maintenance ECT, he had 5-h one-way ground transportation arranged to an out-of-county ECT-equipped facility. There was no relapse in catatonia by the 2-year follow-up. This report highlights a significant healthcare disparity when attempting to manage severe catatonia within community hospital settings without access to ECT in the United States. Alternative treatments, including antipsychotics, had minimal impact on symptoms and possibly increased morbidity in this case while awaiting ECT. Treatment at our designated safety net hospital still required referral to 14 ECT-equipped hospitals before successful transfer. This case highlights the urgent need for ECT availability in more community hospitals to treat patients with refractory psychiatric conditions, including catatonia. ECT is an essential psychiatric treatment that, for certain conditions, has no appropriate alternatives. We propose that access to ECT be considered in the determination of safety net hospital systems, with improved ability to transfer patients who are suffering from treatable life-threatening mental health conditions.</p>","PeriodicalId":75087,"journal":{"name":"The journal of medicine access","volume":"7 ","pages":"27550834231220504"},"PeriodicalIF":1.5000,"publicationDate":"2023-12-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10748610/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The journal of medicine access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/27550834231220504","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
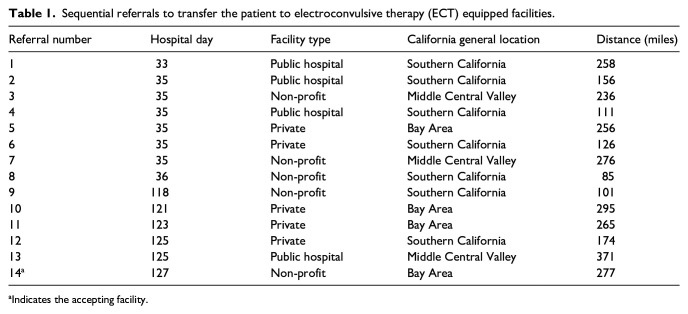
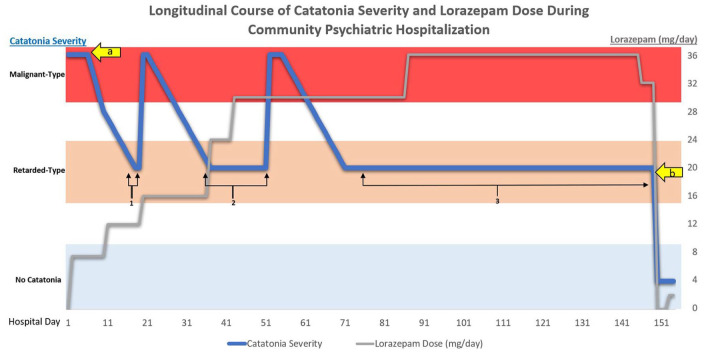
Catatonia is a psychomotor syndrome resulting from an underlying psychiatric or medical disorder commonly observed in inpatient psychiatric units. While benzodiazepines and electroconvulsive therapy (ECT) are effective treatment options, the unavailability of ECT in many community psychiatric hospitals in the United States negatively affects patient outcomes. We present a 25-year-old African American male with a psychiatric diagnosis of schizophrenia complicated by malignant catatonia who was admitted to a community psychiatric hospital. He required intensive medical stabilization with supportive management, and transfer requests to ECT-equipped hospitals were initiated. While awaiting transfer for 148 days, the patient's symptoms did not fully remit with lorazepam (even with 36 mg daily in divided doses) and other psychotropic medication trials, including antipsychotics and mood stabilizers. After nearly 5 months of inpatient stay, he was successfully transferred, received ECT treatment, and experienced rapid resolution of catatonia. After discharge, to obtain three monthly sessions of maintenance ECT, he had 5-h one-way ground transportation arranged to an out-of-county ECT-equipped facility. There was no relapse in catatonia by the 2-year follow-up. This report highlights a significant healthcare disparity when attempting to manage severe catatonia within community hospital settings without access to ECT in the United States. Alternative treatments, including antipsychotics, had minimal impact on symptoms and possibly increased morbidity in this case while awaiting ECT. Treatment at our designated safety net hospital still required referral to 14 ECT-equipped hospitals before successful transfer. This case highlights the urgent need for ECT availability in more community hospitals to treat patients with refractory psychiatric conditions, including catatonia. ECT is an essential psychiatric treatment that, for certain conditions, has no appropriate alternatives. We propose that access to ECT be considered in the determination of safety net hospital systems, with improved ability to transfer patients who are suffering from treatable life-threatening mental health conditions.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


