Building a regional pediatric asthma learning health system in support of optimal, equitable outcomes
Abstract
Introduction
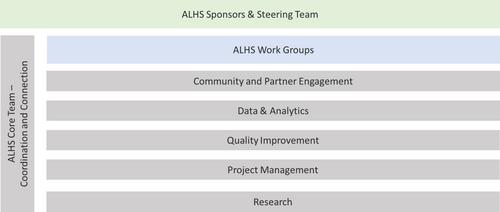
Asthma is characterized by preventable morbidity, cost, and inequity. We sought to build an Asthma Learning Health System (ALHS) to coordinate regional pediatric asthma improvement activities.
Methods
We generated quantitative and qualitative insights pertinent to a better, more equitable care delivery system. We used electronic health record data to calculate asthma hospitalization rates for youth in our region. We completed an “environmental scan” to catalog the breadth of asthma-related efforts occurring in our children's hospital and across the region. We supplemented the scan with group-level assessments and focus groups with parents, clinicians, and community partners. We used insights from this descriptive epidemiology to inform the definition of shared aims, drivers, measures, and prototype interventions.
Results
Greater Cincinnati's youth are hospitalized for asthma at a rate three times greater than the U.S. average. Black youth are hospitalized at a rate five times greater than non-Black youth. Certain neighborhoods bear the disproportionate burden of asthma morbidity. Across Cincinnati, there are many asthma-relevant activities that seek to confront this morbidity; however, efforts are largely disconnected. Qualitative insights highlighted the importance of cross-sector coordination, evidence-based acute and preventive care, healthy homes and neighborhoods, and accountability. These insights also led to a shared, regional aim: to equitably reduce asthma-related hospitalizations. Early interventions have included population-level pattern recognition, multidisciplinary asthma action huddles, and enhanced social needs screening and response.
Conclusion
Learning health system methods are uniquely suited to asthma's complexity. Our nascent ALHS provides a scaffold atop which we can pursue better, more equitable regional asthma outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


