Clinimetric properties of the Perme Intensive Care Unit Mobility Score -a multicenter study for minimum important difference and responsiveness analysis.
Ricardo Kenji Nawa, Marcio Luiz Ferreira De Camillis, Monique Buttignol, Fernanda Machado Kutchak, Eder Chaves Pacheco, Louise Helena Rodrigues Gonçalves, Leonardo Miguel Correa Garcia, Karina Tavares Timenetsky, Luiz Alberto Forgiarini
{"title":"Clinimetric properties of the Perme Intensive Care Unit Mobility Score -a multicenter study for minimum important difference and responsiveness analysis.","authors":"Ricardo Kenji Nawa, Marcio Luiz Ferreira De Camillis, Monique Buttignol, Fernanda Machado Kutchak, Eder Chaves Pacheco, Louise Helena Rodrigues Gonçalves, Leonardo Miguel Correa Garcia, Karina Tavares Timenetsky, Luiz Alberto Forgiarini","doi":"10.25100/cm.v54i3.5580","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of instruments in clinical practice with measurement properties tested is highly recommended, in order to provide adequate assessment and measurement of outcomes.</p><p><strong>Objective: </strong>To calculate the minimum clinically important difference (MCID) and responsiveness of the Perme Intensive Care Unit Mobility Score (Perme Score).</p><p><strong>Methods: </strong>This retrospective, multicentric study investigated the clinimetric properties of MCID, estimated by constructing the Receiver Operating Characteristic (ROC). Maximizing sensitivity and specificity by Youden's, the ROC curve calibration was performed by the Hosmer and Lemeshow goodness-of-fit test. Additionally, we established the responsiveness, floor and ceiling effects, internal consistency, and predictive validity of the Perme Score.</p><p><strong>Results: </strong>A total of 1.200 adult patients records from four mixed general intensive care units (ICUs) were included. To analyze which difference clinically reflects a relevant evolution we calculated the area under the curve (AUC) of 0.96 (95% CI: 0.95-0.98), and the optimal cut-off value of 7.0 points was established. No substantial floor (8.8%) or ceiling effects (4.9%) were observed at ICU discharge. However, a moderate floor effect was observed at ICU admission (19.3%), in contrast to a very low incidence of ceiling effect (0.6%). The Perme Score at ICU admission was associated with hospital mortality, OR 0.86 (95% CI: 0.82-0.91), and the predictive validity for ICU stay presented a mean ratio of 0.97 (95% CI: 0.96-0.98).</p><p><strong>Conclusion: </strong>Our findings support the establishment of the minimum clinically important difference and responsiveness of the Perme Score as a measure of mobility status in the ICU.</p>","PeriodicalId":50667,"journal":{"name":"Colombia Medica","volume":"54 3","pages":"e2005580"},"PeriodicalIF":1.3000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10714681/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Colombia Medica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.25100/cm.v54i3.5580","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of instruments in clinical practice with measurement properties tested is highly recommended, in order to provide adequate assessment and measurement of outcomes.
Objective: To calculate the minimum clinically important difference (MCID) and responsiveness of the Perme Intensive Care Unit Mobility Score (Perme Score).
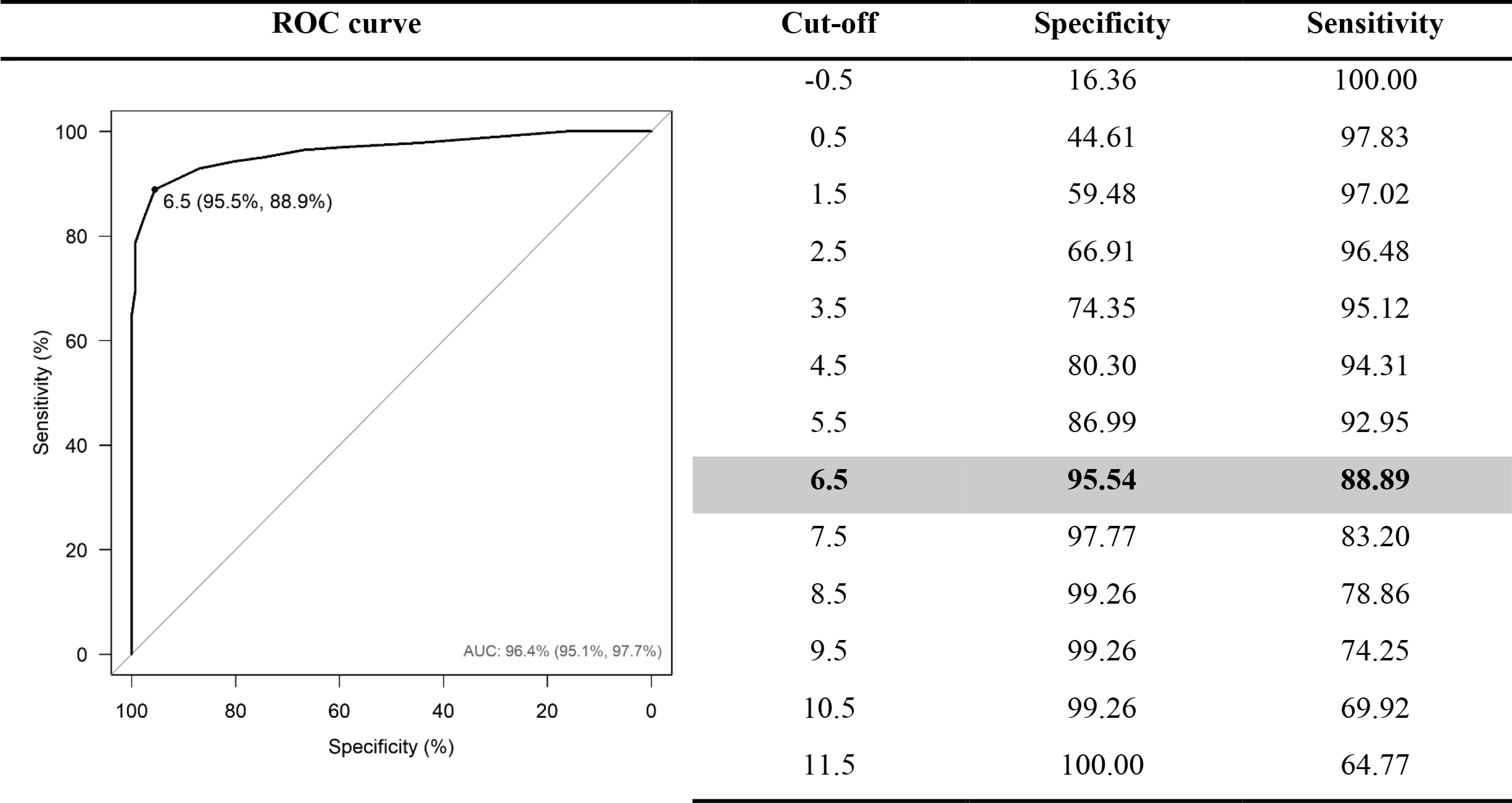
Methods: This retrospective, multicentric study investigated the clinimetric properties of MCID, estimated by constructing the Receiver Operating Characteristic (ROC). Maximizing sensitivity and specificity by Youden's, the ROC curve calibration was performed by the Hosmer and Lemeshow goodness-of-fit test. Additionally, we established the responsiveness, floor and ceiling effects, internal consistency, and predictive validity of the Perme Score.
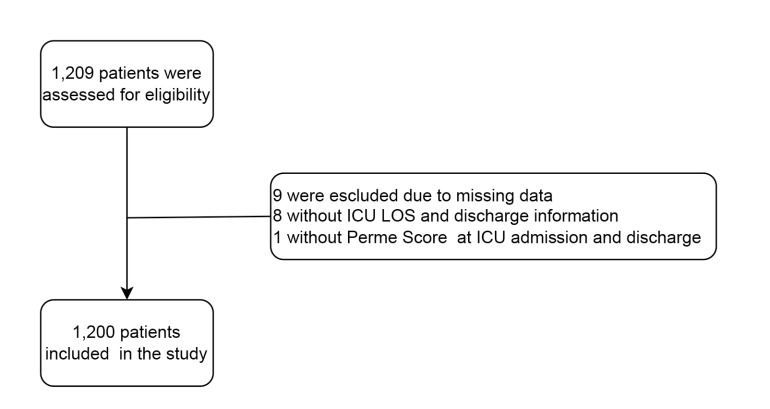
Results: A total of 1.200 adult patients records from four mixed general intensive care units (ICUs) were included. To analyze which difference clinically reflects a relevant evolution we calculated the area under the curve (AUC) of 0.96 (95% CI: 0.95-0.98), and the optimal cut-off value of 7.0 points was established. No substantial floor (8.8%) or ceiling effects (4.9%) were observed at ICU discharge. However, a moderate floor effect was observed at ICU admission (19.3%), in contrast to a very low incidence of ceiling effect (0.6%). The Perme Score at ICU admission was associated with hospital mortality, OR 0.86 (95% CI: 0.82-0.91), and the predictive validity for ICU stay presented a mean ratio of 0.97 (95% CI: 0.96-0.98).
Conclusion: Our findings support the establishment of the minimum clinically important difference and responsiveness of the Perme Score as a measure of mobility status in the ICU.
期刊介绍:
Colombia Médica is an international peer-reviewed medical journal that will consider any original contribution that advances or illuminates medical science or practice, or that educates to the journal''s’ readers.The journal is owned by a non-profit organization, Universidad del Valle, and serves the scientific community strictly following the International Committee of Medical Journal Editors (ICMJE) and the World Association of Medical Editors (WAME) recommendations of policies on publication ethics policies for medical journals.
Colombia Médica publishes original research articles, viewpoints and reviews in all areas of medical science and clinical practice. However, Colombia Médica gives the highest priority to papers on general and internal medicine, public health and primary health care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


