Sant Kumar, Nayrana Griffith, Dylan Walter, Michael Swett, Venkatesh Raman, Jose D Vargas, Brototo Deb, Jiling Chou, Ayah Arafat, Monvadi B Srichai
{"title":"Characterization of Myocardial Injury With High-Sensitivity Troponin.","authors":"Sant Kumar, Nayrana Griffith, Dylan Walter, Michael Swett, Venkatesh Raman, Jose D Vargas, Brototo Deb, Jiling Chou, Ayah Arafat, Monvadi B Srichai","doi":"10.14503/THIJ-23-8108","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-sensitivity troponin I, cardiac form (hs-cTnI) accelerates the assessment of acute coronary syndrome. Little has been documented about its performance, how it relates to different types of myocardial injury, and its impact on morbidity and mortality. This study sought to expand understanding of hs-cTnI by characterizing types of myocardial injury, the impact of comorbidities, and 30-day outcomes.</p><p><strong>Methods: </strong>The study retrospectively evaluated 1,975 patients with hs-cTnI levels obtained in the emergency department or inpatient setting from June to September 2020. Troponin was considered elevated if it was higher than the 99th percentile for either sex. Charts were reviewed to determine the presence of myocardial injury. Troponin elevation was adjusted for demographics, comorbidities, and kidney dysfunction. Thirty-day mortality and readmission rates were calculated.</p><p><strong>Results: </strong>Of 1,975 patients, 468 (24%) had elevated hs-cTnI, and 330 (17%) had at least 1 type of myocardial injury, type 2 myocardial infarction being the most frequent. Sensitivity and specificity using the 99th percentile as a cutoff were 99% and 92%, respectively. The average maximum hs-cTnI level was significantly higher for type 1 myocardial infarction (P < .001). Being male, Black, non-Hispanic, and a hospital inpatient were all associated with higher initial and peak hs-cTnI levels (P < .001). Elevated hs-cTnI level, age, heart disease, kidney dysfunction, and inpatient status were predictive of 30-day mortality on multivariate analysis.</p><p><strong>Conclusion: </strong>Elevated hs-cTnI levels in emergency department and inpatient settings occurs most commonly because of type 2 myocardial infarction. Maximum hs-cTnI level is associated with the patient's particular type of myocardial injury, certain demographics, and cardiovascular comorbidities, and it may be a predictor of 30-day outcomes.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"50 6","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2023-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10751476/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8108","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: High-sensitivity troponin I, cardiac form (hs-cTnI) accelerates the assessment of acute coronary syndrome. Little has been documented about its performance, how it relates to different types of myocardial injury, and its impact on morbidity and mortality. This study sought to expand understanding of hs-cTnI by characterizing types of myocardial injury, the impact of comorbidities, and 30-day outcomes.
Methods: The study retrospectively evaluated 1,975 patients with hs-cTnI levels obtained in the emergency department or inpatient setting from June to September 2020. Troponin was considered elevated if it was higher than the 99th percentile for either sex. Charts were reviewed to determine the presence of myocardial injury. Troponin elevation was adjusted for demographics, comorbidities, and kidney dysfunction. Thirty-day mortality and readmission rates were calculated.
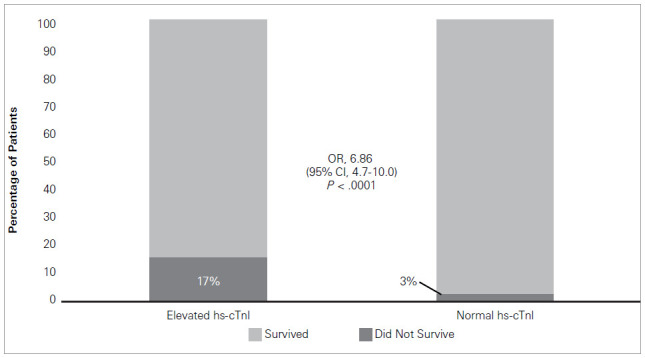
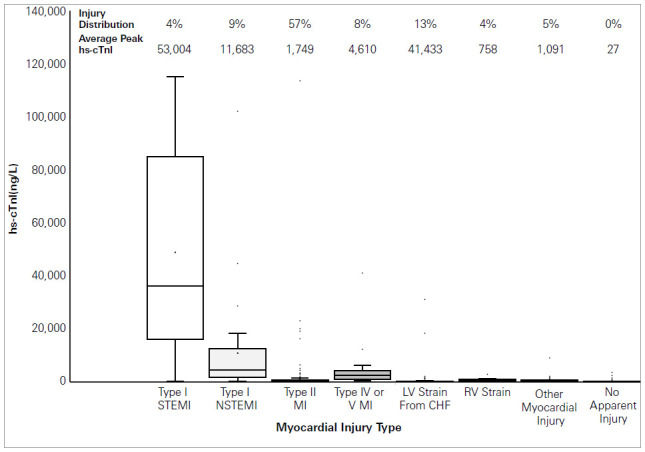
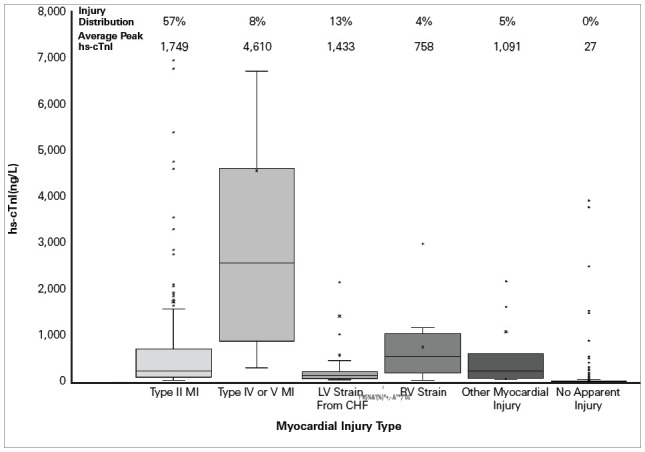
Results: Of 1,975 patients, 468 (24%) had elevated hs-cTnI, and 330 (17%) had at least 1 type of myocardial injury, type 2 myocardial infarction being the most frequent. Sensitivity and specificity using the 99th percentile as a cutoff were 99% and 92%, respectively. The average maximum hs-cTnI level was significantly higher for type 1 myocardial infarction (P < .001). Being male, Black, non-Hispanic, and a hospital inpatient were all associated with higher initial and peak hs-cTnI levels (P < .001). Elevated hs-cTnI level, age, heart disease, kidney dysfunction, and inpatient status were predictive of 30-day mortality on multivariate analysis.
Conclusion: Elevated hs-cTnI levels in emergency department and inpatient settings occurs most commonly because of type 2 myocardial infarction. Maximum hs-cTnI level is associated with the patient's particular type of myocardial injury, certain demographics, and cardiovascular comorbidities, and it may be a predictor of 30-day outcomes.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


