{"title":"Complete recovery after glucocorticoid replacement therapy in a case of primary adrenal insufficiency caused by adrenal tuberculosis infection.","authors":"Hendra Zufry, Putri Oktaviani Zulfa, Rosdiana Rosdiana, Krishna Wardhana Sucipto, Agustia Sukri Ekadamayanti, Sarah Firdausa","doi":"10.1530/EDM-23-0112","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>Symptoms of primary adrenal insufficiency (PAI) are commonly nonspecific, causing the disease to be misdiagnosed or often delayed, and patients may present to the hospital with a life-threatening crisis. Previous case reports have documented that patients in this condition often require lifelong glucocorticoid replacement therapy. This study aimed to present a noteworthy outcome of PAI caused by adrenal tuberculosis infection, demonstrating complete recovery after six months of glucocorticoid replacement therapy. A 38-year-old Indonesian man presented to the endocrinology clinic in a tertiary hospital with a chief complaint of epigastric pain. The patient experienced nausea, vomiting, loss of consciousness, weight loss, excessive sweat, decreased appetite, weakness, and dizziness in the past 2 weeks. Laboratory examinations revealed hyponatremia, elevated adrenocorticotropic hormone, and suppressed morning plasma cortisol level. A non-contrast-enhanced abdominal MRI showed unilateral right-side adrenal enlargement and calcification. The patient's Mantoux test was positive. Corticosteroids and anti-tuberculosis therapy were administered. After 6 months, hydrocortisone was discontinued due to the patient's good clinical condition and normal morning plasma cortisol levels. After a 1-year follow-up, the patient remained asymptomatic with normal cortisol levels. We hypothesized several reasons for this unique outcome: (i) the patient was relatively young compared to previous cases, suggesting an adequate immune system may play a role; (ii) despite a 1-month delay in diagnosis and treatment, the absence of skin hyperpigmentation suggested an acute presentation, potentially contributing to the favorable outcome; and (iii) the absence of comorbidities potentially positively impacted the patient's outcome.</p><p><strong>Learning points: </strong>Symptoms of adrenal insufficiency are often nonspecific and may only become apparent once significant damage has occurred to the adrenal gland. Clinical adjustments and a comprehensive understanding of epidemiological knowledge are necessary for diagnosing patients with endocrine diseases in limited-resource settings. Complete recovery in primary adrenal insufficiency caused by tuberculosis infection might be due to younger age, acute presentation, and absence of comorbidities.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2023 4","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2023-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10762589/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-23-0112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
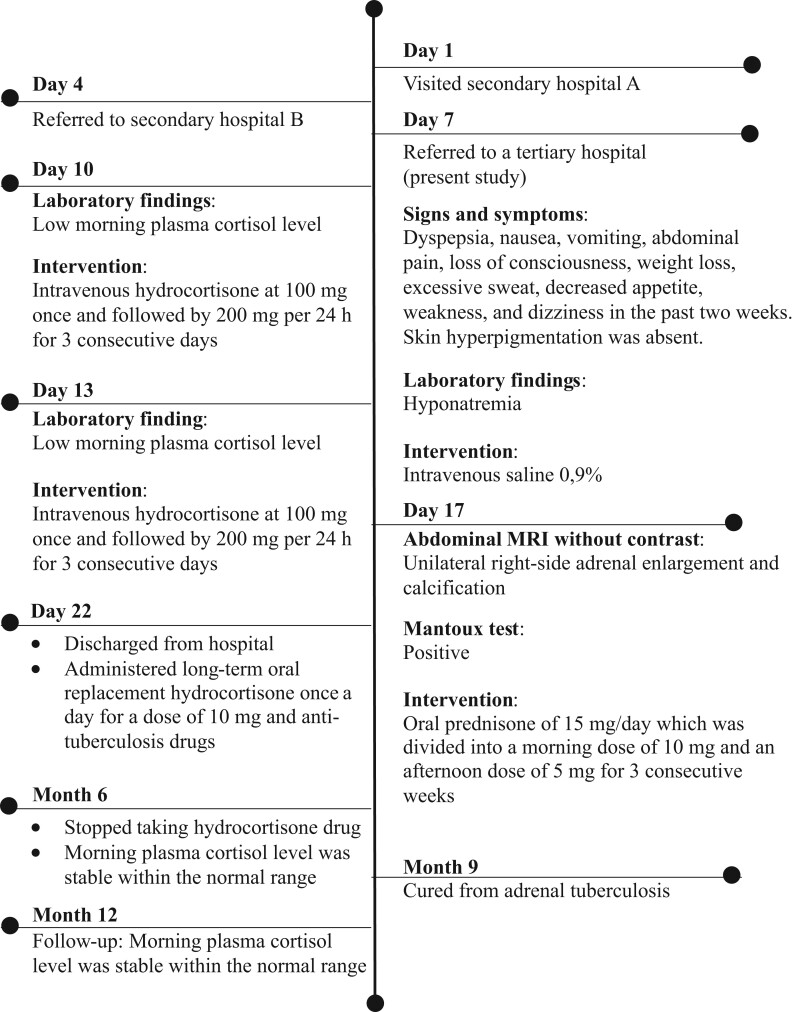
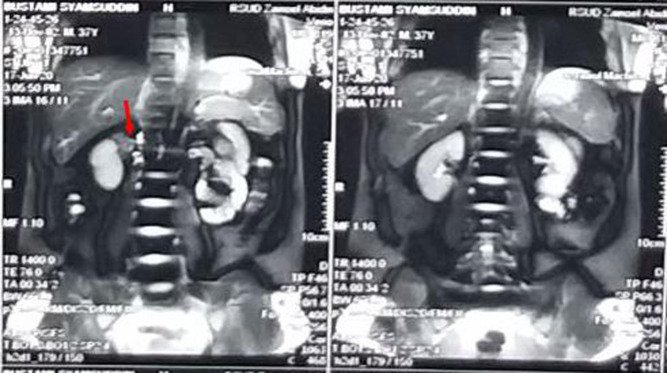
Summary: Symptoms of primary adrenal insufficiency (PAI) are commonly nonspecific, causing the disease to be misdiagnosed or often delayed, and patients may present to the hospital with a life-threatening crisis. Previous case reports have documented that patients in this condition often require lifelong glucocorticoid replacement therapy. This study aimed to present a noteworthy outcome of PAI caused by adrenal tuberculosis infection, demonstrating complete recovery after six months of glucocorticoid replacement therapy. A 38-year-old Indonesian man presented to the endocrinology clinic in a tertiary hospital with a chief complaint of epigastric pain. The patient experienced nausea, vomiting, loss of consciousness, weight loss, excessive sweat, decreased appetite, weakness, and dizziness in the past 2 weeks. Laboratory examinations revealed hyponatremia, elevated adrenocorticotropic hormone, and suppressed morning plasma cortisol level. A non-contrast-enhanced abdominal MRI showed unilateral right-side adrenal enlargement and calcification. The patient's Mantoux test was positive. Corticosteroids and anti-tuberculosis therapy were administered. After 6 months, hydrocortisone was discontinued due to the patient's good clinical condition and normal morning plasma cortisol levels. After a 1-year follow-up, the patient remained asymptomatic with normal cortisol levels. We hypothesized several reasons for this unique outcome: (i) the patient was relatively young compared to previous cases, suggesting an adequate immune system may play a role; (ii) despite a 1-month delay in diagnosis and treatment, the absence of skin hyperpigmentation suggested an acute presentation, potentially contributing to the favorable outcome; and (iii) the absence of comorbidities potentially positively impacted the patient's outcome.
Learning points: Symptoms of adrenal insufficiency are often nonspecific and may only become apparent once significant damage has occurred to the adrenal gland. Clinical adjustments and a comprehensive understanding of epidemiological knowledge are necessary for diagnosing patients with endocrine diseases in limited-resource settings. Complete recovery in primary adrenal insufficiency caused by tuberculosis infection might be due to younger age, acute presentation, and absence of comorbidities.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


