Jennifer Chia-Ying Chung, Nitish Bhatt, Louis-Mathieu Stevens, Rashmi Nedadur, Marina Ibrahim, Kiera Liblik, Michael W A Chu, Maral Ouzounian
{"title":"Trends in sex-specific differences following aortic arch repair: results from the Canadian Thoracic Aortic Collaborative.","authors":"Jennifer Chia-Ying Chung, Nitish Bhatt, Louis-Mathieu Stevens, Rashmi Nedadur, Marina Ibrahim, Kiera Liblik, Michael W A Chu, Maral Ouzounian","doi":"10.21037/acs-2023-adw-0163","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous data have shown that sex-related differences exist in aortic arch surgery, with female patients experiencing worse outcomes. Over time, as surgical techniques and strategies have improved, these improvements have benefitted female patients. Using a multicenter national aortic registry from the Canadian Thoracic Aortic Collaborative (CTAC), we aimed to determine the relationship between sex and outcomes following aortic arch repair and to examine how these have changed over time.</p><p><strong>Methods: </strong>The multicenter prospective CTAC database of all aortic procedures performed under circulatory arrest from participating centers across Canada (n=9) was used. Patients were included who underwent elective or urgent/emergency arch reconstruction under circulatory arrest from 2002 to 2021. The primary composite endpoint was defined as the occurrence of one of the following endpoints: in-hospital mortality, stroke, dialysis-dependent renal failure, deep sternal wound infection, reoperation, or prolonged ventilation of >40 hours. Secondary endpoints included in-hospital mortality, in-hospital stroke, and a modified version of the Society of Thoracic Surgeons-defined composite endpoint for mortality and major morbidity (MMOM).</p><p><strong>Results: </strong>A total of 2,592 patients who underwent aortic arch repair between 2002 and 2021 (31.4% female and 68.6% male patients). Operative mortality decreased through the study period for female patients. No change in operative mortality was observed in male patients or following elective repair. The composite endpoint improved for female patients over time in both elective and urgent surgery, while for male patients, rates improved for elective surgery and remained stable for urgent. Ultimately, female sex was not an independent predictor of adverse outcomes following aortic arch repair.</p><p><strong>Conclusions: </strong>Our results are congruent with existing data and are highly encouraging. It shows that multilevel improvements in our approach to aortic arch surgery have helped to serve female patients who were previously disadvantaged.</p>","PeriodicalId":8067,"journal":{"name":"Annals of cardiothoracic surgery","volume":"12 6","pages":"558-568"},"PeriodicalIF":3.1000,"publicationDate":"2023-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10711408/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of cardiothoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/acs-2023-adw-0163","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Previous data have shown that sex-related differences exist in aortic arch surgery, with female patients experiencing worse outcomes. Over time, as surgical techniques and strategies have improved, these improvements have benefitted female patients. Using a multicenter national aortic registry from the Canadian Thoracic Aortic Collaborative (CTAC), we aimed to determine the relationship between sex and outcomes following aortic arch repair and to examine how these have changed over time.
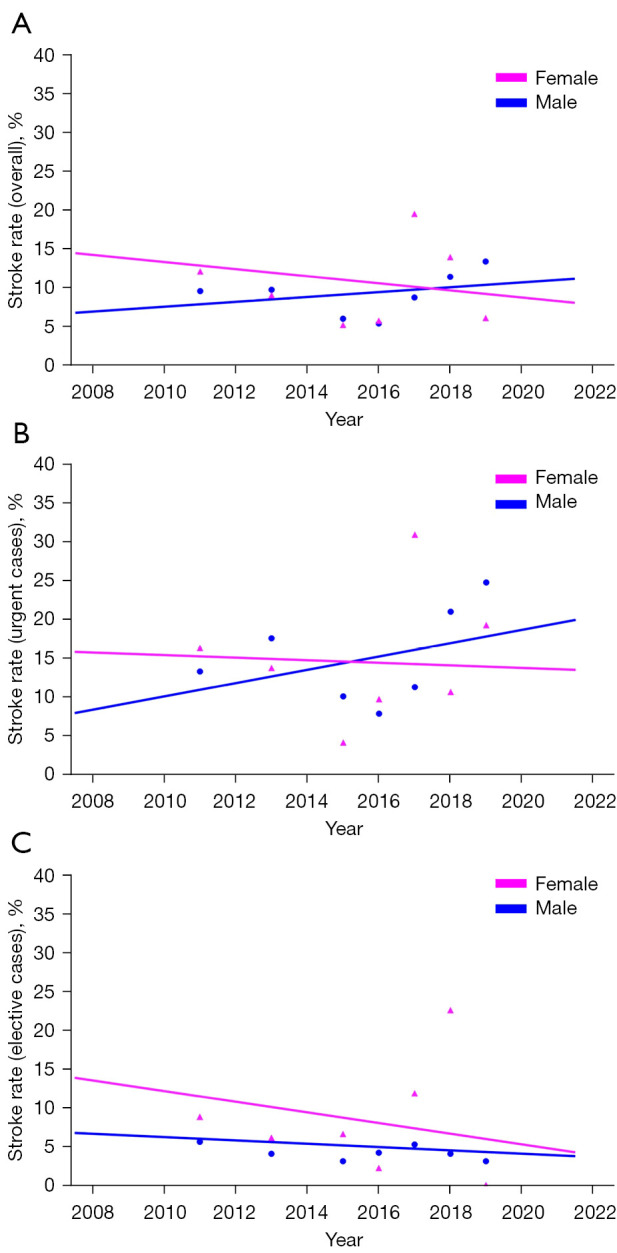
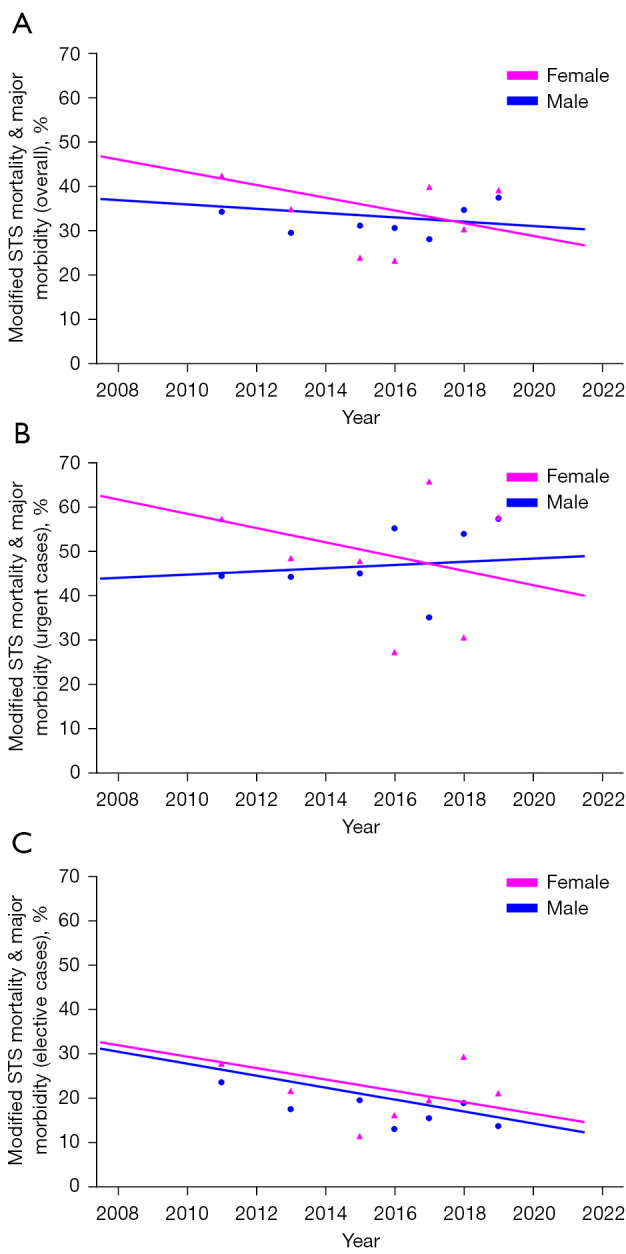
Methods: The multicenter prospective CTAC database of all aortic procedures performed under circulatory arrest from participating centers across Canada (n=9) was used. Patients were included who underwent elective or urgent/emergency arch reconstruction under circulatory arrest from 2002 to 2021. The primary composite endpoint was defined as the occurrence of one of the following endpoints: in-hospital mortality, stroke, dialysis-dependent renal failure, deep sternal wound infection, reoperation, or prolonged ventilation of >40 hours. Secondary endpoints included in-hospital mortality, in-hospital stroke, and a modified version of the Society of Thoracic Surgeons-defined composite endpoint for mortality and major morbidity (MMOM).
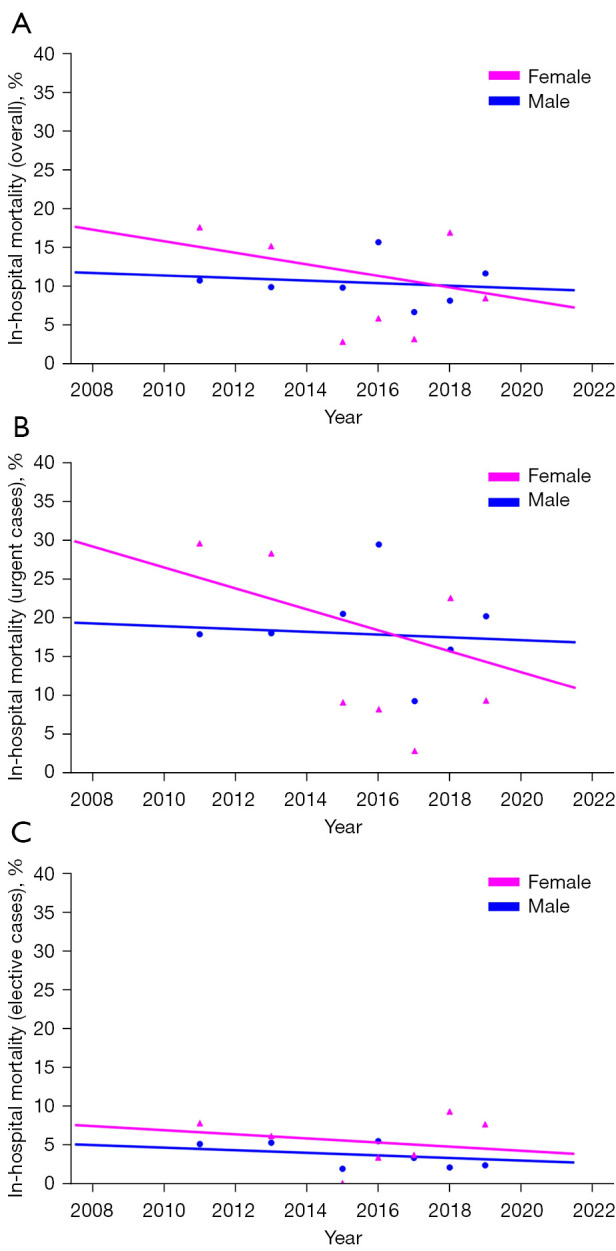
Results: A total of 2,592 patients who underwent aortic arch repair between 2002 and 2021 (31.4% female and 68.6% male patients). Operative mortality decreased through the study period for female patients. No change in operative mortality was observed in male patients or following elective repair. The composite endpoint improved for female patients over time in both elective and urgent surgery, while for male patients, rates improved for elective surgery and remained stable for urgent. Ultimately, female sex was not an independent predictor of adverse outcomes following aortic arch repair.
Conclusions: Our results are congruent with existing data and are highly encouraging. It shows that multilevel improvements in our approach to aortic arch surgery have helped to serve female patients who were previously disadvantaged.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


