{"title":"New insights on diagnosis and treatment of AVP deficiency","authors":"Julie Refardt, Cihan Atila, Mirjam Christ-Crain","doi":"10.1007/s11154-023-09862-w","DOIUrl":null,"url":null,"abstract":"<p>Arginine vasopressin deficiency (AVP-D) is one of the main entities of the polyuria-polydipsia syndrome. Its correct diagnosis and differentiation from the other two causes - AVP resistance and primary polydipsia – is crucial as this determines the further management of these patients.</p><p>Over the last years, several new diagnostic tests using copeptin, the stable surrogate marker of AVP, have been introduced. Among them, hypertonic saline stimulated copeptin was confirmed to reliably and safely improve the diagnostic accuracy to diagnose AVP-D. Due to its simplicity, arginine stimulated copeptin was put forward as alternative test procedure. Glucagon-stimulated copeptin also showed promising results, while the oral growth hormone secretagogue Macimorelin failed to provide a sufficient stimulus. Interestingly, an approach using machine learning techniques also showed promising results concerning diagnostic accuracy.</p><p>Once AVP-D is diagnosed, further workup is needed to evaluate its etiology. This will partly define the further treatment and management. In general, treatment of AVP-D focuses on desmopressin substitution, with oral formulations currently showing the best tolerance and safety profile. However, in addition to desmopressin substitution, recent data also showed that psychopathological factors play an important role in managing AVP-D patients.</p>","PeriodicalId":21105,"journal":{"name":"Reviews in Endocrine and Metabolic Disorders","volume":"32 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reviews in Endocrine and Metabolic Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11154-023-09862-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
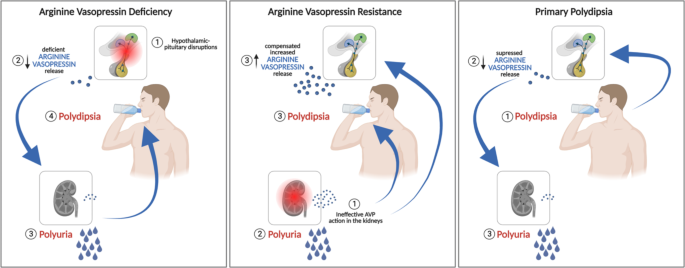
Arginine vasopressin deficiency (AVP-D) is one of the main entities of the polyuria-polydipsia syndrome. Its correct diagnosis and differentiation from the other two causes - AVP resistance and primary polydipsia – is crucial as this determines the further management of these patients.
Over the last years, several new diagnostic tests using copeptin, the stable surrogate marker of AVP, have been introduced. Among them, hypertonic saline stimulated copeptin was confirmed to reliably and safely improve the diagnostic accuracy to diagnose AVP-D. Due to its simplicity, arginine stimulated copeptin was put forward as alternative test procedure. Glucagon-stimulated copeptin also showed promising results, while the oral growth hormone secretagogue Macimorelin failed to provide a sufficient stimulus. Interestingly, an approach using machine learning techniques also showed promising results concerning diagnostic accuracy.
Once AVP-D is diagnosed, further workup is needed to evaluate its etiology. This will partly define the further treatment and management. In general, treatment of AVP-D focuses on desmopressin substitution, with oral formulations currently showing the best tolerance and safety profile. However, in addition to desmopressin substitution, recent data also showed that psychopathological factors play an important role in managing AVP-D patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


